
Hype Cycle for U.S. Healthcare Payers, 2017
This Hype Cycle tracks the maturity and adoption rates of emerging technologies that are important to healthcare payers' digital transformation. CIOs can use this note to prioritize, create roadmaps and coordinate initiatives with their peers and partners to enable critical business capabilities.
Analysis
What You Need to Know
Healthcare payers are facing a defining moment at the intersection of industry tumult and digital disruption. Gartner's health-value management business model lays out a rationale and architecture for transformation spanning business capabilities from intelligent administration to applied business intelligence (BI)/analytics, to provider and purchaser alignment, and to population health and consumer engagement management.
This Hype Cycle tracks the maturity and adoption rates of the important technologies that enable those capabilities. It is designed to help you play a pivotal role (along with your teams and business partners) in planning and prioritizing a technology roadmap, as well as collaborating and advancing IT's contribution to your organization's future performance. Prepare now to apply a wave of emerging analytics and consumer engagement innovations to increase your organization's value to your end customers.
The Hype Cycle
The multitude of challenges that payers face in 2017 have a bright side as investment capital and sound ideas are flowing into IT solutions that are designed to help.
This updated Hype Cycle specifically reflects technology developments that respond to the critical forces in the industry. It also includes new profiles that address the demands of accountable care organization (ACO) collaboration and associated value-based payment reforms, the urgency to address nonmedical determinants of health, consumers' adoption of virtual care and nontraditional engagement channels, the convergence of administrative and clinical consumer services, and clinical data exchange.
The most important underlying digital technology forces reflected in these new profiles are modern BI and data science architecture (including artificial intelligence), the Internet of Things, ecosystem-enabling cross-sector and cross-industry data connections and workflows (platforms), and the emerging member engagement hub (intelligence plus connections).
All industry Hype Cycles feature technologies that address the requirements and opportunities specific to their unique operating contexts. No healthcare CIOs can succeed if they do not also understand and respond to those capabilities being implemented by the business partners with whom their success is intertwined. Accordingly, we present here select, critical emerging technologies that your providers/partners are implementing. These include both Genomics Medicine and Precision Medicine from our "Hype Cycle for Healthcare Providers, 2017." Both of these developing capabilities will eventually redefine what constitutes quality care with major analytics, payment, consumer engagement and marketing implications for payers.
We also track Blockchain in Healthcare technology, which, while still in its infancy in solving a meaningful payer problem, generally holds both hope and promise in helping to address healthcare's complex transactional and data aggregation/sharing problems. We also include the Health Data Convergence Hub, a category focused on data integration and exchange across partners in healthcare.
Please note: This research is not intended to be used on its own. Absent the context of the business drivers that make these capabilities valuable, this is just cool stuff. Furthermore, not all of these technologies will be useful to your business in their current state. But with our evidence-based analysis combined with your thoughtful assessments, your well-timed investments in these developing technologies are more likely to pay off.
Figure 1. Hype Cycle for U.S. Healthcare Payers, 2017
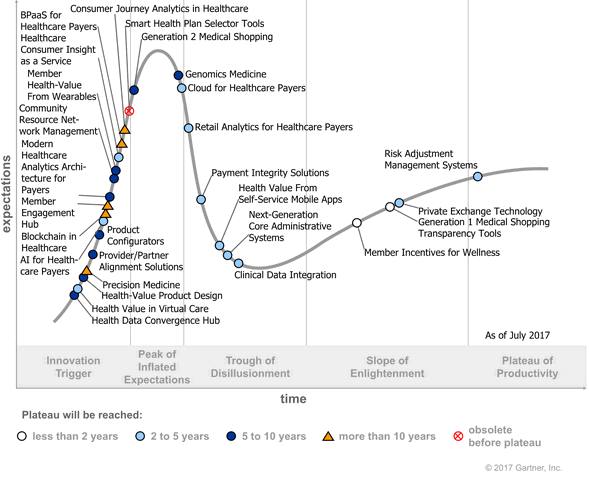
Source: Gartner (July 2017)
The Priority Matrix
The Priority Matrix is a companion to the Hype Cycle graphic. It plots the answers to two key questions: (1) How much value could your organization expect to realize from the effective implementation of a particular technology? (2) When will the technology be mature enough to help deliver that value?
Taking a broad view of this matrix, it's evident that there is no panacea technology for payers' pressing problems. Transformational technologies are five to 10 years out. However, note the prevalence of profiles of high to moderate value in the time frame of two years or more. That means 2017 is the right time to be focusing on leveraging the cloud, achieving scale in clinical data integration (CDI), scaling up your analytics capabilities, and modernizing your core to free up resources for further innovation on the foreseeable horizon.
Also, avoid distractions. While blockchain's allure has increased, the practical use cases for payers remain elusive and, hence, years away. Rather, emerging capabilities in Healthcare Consumer Insight as a Service and Member Engagement Hub present planning and preparation opportunities now to accelerate customer engagement and population health management. Likewise, Payment Integrity Solutions and Next-Generation Core Administrative Systems should be on your list for delivering near-term savings and operating efficiency.
In the Priority Matrix, the quickly maturing transformational technologies are up and to the left. Below them are important technologies with a lesser scope of potential impact. Look to the right and you will find emerging technologies with great potential that are further away from their full maturity. Below these are technologies with a lesser scope of impact. Expect our "benefit" plotting of technologies (farther to the right) to change over time. Hold us to the benefit judgments in the nearer term. Use your judgment, plus ours, to make smart investment and implementation decisions.
Figure 2. Priority Matrix for U.S. Healthcare Payers, 2017
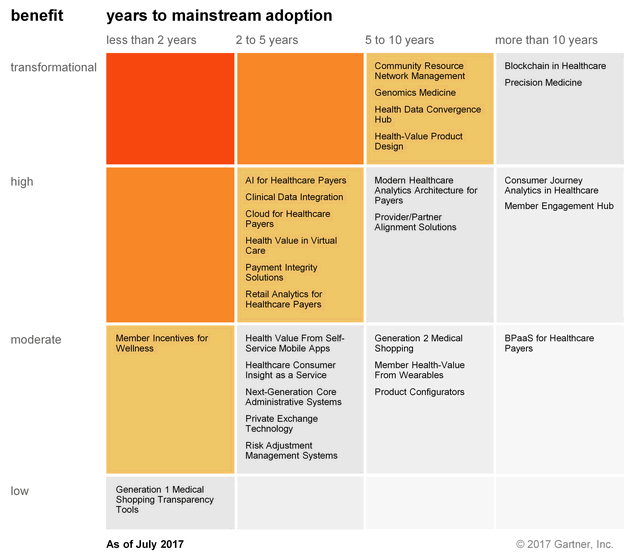
Source: Gartner (July 2017)
Off the Hype Cycle
We have made the following changes to this year's Hype Cycle:
Removed:
- Risk-Bearing Provider Entities: While the ACO trend continues and is a significant driver of payers' need to partner more effectively with providers, we more specifically address the technology implications for payers of this trend in our updated Provider Network Management Applications profile, now renamed the Provider/Partner Alignment Solutions profile, and in the new Health Data Convergence Hub and Modern Healthcare Analytics Architecture for Payers profiles.
- B2C Technology Strategies: This category has been explored more deeply in the Member Health-Value From Wearables, Health Value in Virtual Care, Health Value From Self-Service Mobile Apps, Health-Value Product Design and other consumer engagement technologies in the Hype Cycle.
Consolidated: When we initiated the profile on Sales Channel Performance Analytics in the early years of the U.S. Affordable Care Act's (ACA's) implementation, payers were actively developing analytics to better understand the impact of ACA on various sales channels — especially the cost of sales across direct online, marketplace and broker-facilitated sales. More recently, analytics oriented around members and prospects have subsumed those earlier efforts, and applied concepts like "member next-best action" and "member lifetime value" across all members in all lines of business. This new orientation is covered in the Retail Analytics for Healthcare Payers profile.
As we have tracked payers' adoption of outsourcing in our broad BPO Strategy profile, which has accelerated into the mainstream, the major core administrative processing solutions (CAPS) vendors of industry-specific services have likewise accelerated their shift toward the cloud and into BPaaS for Healthcare Payers technology. Rather than tracking these separately, we have shifted our research focus to payers' growing interest in and emerging embrace of outsourcing through BPaaS.
BPM is a maturing technology that is now covered in this Hype Cycle as part of Provider/Partner Alignment Solutions, Member Engagement Hub and Community Resource Network Management. In addition, Automated Provider Payment and Automated Premium Billing are both part of the expanded Next-Generation Core Administrative Systems profile.
Graduated: Gartner has also removed the following profiles from the Hype Cycle:
- Health and Wellness Systems have reached mainstream adoption. Most payers have implemented (on their own, or at the insistence of a self-funded employer group) some version of a homegrown or vended capability to engage members in their care and ongoing wellness, often with incentives for participation or compliance.
- Care Management Analytics have also matured to the point of mainstream adoption, and are now an established competency for most payers.
On the Rise
Blockchain in Healthcare
Analysis By: Gregg Pessin
Definition: Blockchain is a type of distributed ledger in which transactions are sequentially grouped into blocks. Each block is chained to the previous block and immutably recorded across a peer-to-peer network, using cryptographic trust and assurance mechanisms. Depending on the implementation, transactions can include programmable behavior. Healthcare blockchain encompasses all practical applications of this technology within the industry.
Position and Adoption Speed Justification: Healthcare CIOs are abuzz about the potential business processes that could be streamlined or replaced by blockchain-enabled alternatives. Early blockchain implementations in financial services have spurred the healthcare hype. Top of the list are processes that are subject to fraud, or that depend on interoperability and high degrees of security. However, essential underpinnings like data standards and structures are major impediments. Issues of scalability, health-data-specific security and adherence to existing regulations further cloud the picture. Nonetheless, because most blockchain initiatives are based on open-source technology, innovation and evolution will happen quickly.
In 2017, it's clear the healthcare blockchain is still in its infancy. Although blockchain is in the top 10 search list by clients at Gartner, fewer than 5% of healthcare provider CIOs and only 12% in the payer industry have blockchain in their roadmaps, and even fewer are actually working on funded projects, today.
Healthcare clients are unsure of how to best pursue a blockchain strategy, considering there are so few viable commercial models. Clients express uncertainty about blockchain's fit into their mature exchange, maturing supply chain, evolving data sharing and customer engagement strategies, and are unsure when blockchain will be ready. There are several governance styles for blockchain that are still unfolding within healthcare: (1) a public-permissionless model (such as bitcoin technology stack); (2) a private-permissioned environment that leverages a consensus model; (3) a hybrid-permissioned environment, where the consensus model is provided by a third party; and (4) a private permissioned environment where the consensus model is operated by an institution for it and its partners.
In the payer and provider worlds, the speculation is focused on streamlining transactions and data sharing among all the major players in the healthcare value chain for everything from contracting, credentialing and claims payment, to health data aggregation and analysis, and population health management. Also, longitudinal medical records could be the source for precision medicine and population health studies.
Today, there are very few vendors, IT consultant firms, and sponsor organizations that understand block chain and have healthcare industry experience and deep business domain expertise (e.g., supply chain, R&D, claims adjudication or EHR/EMR).
User Advice: Distributed ledger concepts are complex and are not well-understood by the healthcare CIO community. Existing production examples of blockchain such as bitcoin are useful to understand and explain the concepts and underlying technologies.
Progress is being made by several vendors to develop distributed ledgers for medical information storage. At least eight startups are underway for this purpose. Tracking those vendors is a smart step.
To fully keep abreast of this emerging technology:
- Assign personnel to research and identify applicable use cases as potential candidates for pilots or proofs of concept.
- Recognize that the terminology surrounding blockchain is in flux. This uncertainty masks the potential suitability of technology solutions to meet business use cases. Use caution when interacting with vendors that have ill-defined/nonexistent blockchain offerings.
- As you plan, ensure you are clearly identifying how the term "blockchain" is being used and applied, both internally and by providers, in order to better understand the costs and returns compared to existing "proven" technologies.
- Proactively explore the four styles of governance as part of your organization's strategic planning efforts, especially as they relate to specific business use cases and operational risk assessments.
- Monitor the evolution of blockchain, including related initiatives, such as consensus mechanism development, sidechains and distributed ledger.
- Monitor the vendors that are marketing their solutions. Vendors are currently peddling concepts with few active POCs.
Business Impact: Blockchain and distributed-ledger concepts are gaining traction with healthcare businesses because they hold the promise of transforming both architectures and operating models. However, the business case for block chain in healthcare is still an open book.
Now is the time for industry stakeholders to learn from and then build upon existing models as they evolve. The potential of this technology to radically transform economic interactions should also raise critical questions for health value chain, regulators, suppliers, patients and consumers, for which there are no clear answers today.
As healthcare companies get more serious about blockchain, it will become critical to ensure that the right type of governance is applied in order to drive innovation, collaboration and more efficient supply chains. The benefits, if the technology can be applied correctly, are very clear. Block chain will enable efficiencies for reaching new customers, extending relationships with supply chain partners, and offering better quality and more complete links between events. It should expand the boundaries of healthcare businesses.
Benefit Rating: Transformational
Market Penetration: Less than 1% of target audience
Maturity: Embryonic
Sample Vendors: Blockchain Health; Brontech; Gem; Guardtime; Hashed Health; HealthCombix; MedRec; PointNurse; PokitDok
Health Data Convergence Hub
Analysis By: Laura Craft
Definition: The health data convergence hub is the orchestration platform that brings together data from across the consumer/citizen/patient health and wellness continuum and prepares the data for delivery to downstream consumption platforms, applications, analytics and "things." It automates the ingestion of data — both structured and unstructured — from all identified and permissioned sources; provides tracking and traceability; and manages identity, compliance and security. It may process algorithms and deliver the output to the correct modality.
Position and Adoption Speed Justification: This technology profile acknowledges that the vast amounts of data that are becoming essential to sustain health and wellness, contain healthcare costs, and make sure the customer/patient/person is engaged and satisfied are becoming an enormous and daunting integration undertaking. The assessment of health and health risk is now relying on data sources that historically have been beyond the reach of the healthcare delivery organization, such as social determinants of health and genomic profile data. In addition, delivery of care is coordinated across an integrated community network and to help facilitate patient compliance, which includes broadening services like coordination of transportation and delivery of food. The result is an expanding ecosystem of care coordination and data exchange. The data needed to support all the healthcare actions is often needed in real time and is typically an aggregation of many data points to provide the holistic picture of the patient. This broadening ecosystem of data collection, sharing and delivery taxes traditional data exchange integration methods (HIEs and ETLs) that have been implemented for purpose-specific reasons and are less effective to manage to new data demands. Healthcare delivery organizations that are truly executing population health management will quickly feel the gaps, bottlenecks and delays created by poor data movement. The health data convergence hub, which is distinctly different from an HIE (but may rely on one as a source of information) and ETL tools, is also critical to HDOs' real-time and digital healthcare strategies.
There are two approaches emerging in the industry. The first emerges from existing analytic and population health platform players that historically have been the integrators of bringing the disparate data together. Gartner has noted that some of the large, well-established population health/analytic vendors like Health Catalyst are retooling their platforms to have more powerful ingestion and data management strengths. The second approach is a new, emerging class of vendors. These vendors may have tangential solutions to support population health and analytics, but have as the primary focus of the solution data ingestion, indexing and distribution. This is their core differentiator and strength. One example is Imat Solutions, which aggregates, normalizes, indexes and codifies all patient data from across the continuum of care to make it consumable. DataMotionHealth is another example. The compelling difference of these vendors is the expertise brought to this highly challenging layer of the architecture.
We position health data convergence hubs at post-trigger 10%, as the solutions are still early attempts to build a hub that effectively transacts, normalizes and orchestrates real-time patient/consumer/citizen data regardless of origin or destination. Limitations driven by the lack of better industry standards may impact progress as well as adoption. However, Gartner believes that within 5 to 10 years, this will be a powerful (and standard) layer of the HDO's enterprise architecture.
User Advice: Healthcare CIOs must make sure they do not become the cause of integration and data challenges and become a bottleneck to organizational progress and transformation:
- Get ahead of the need by proactively understanding what the data integration demands across the healthcare delivery organization will be over the next three to five years. These needs can be culled from information in the organization's strategic plan and through other deliberate short- and long-term visioning exercises.
- Create requirements. Map out the patient, provider and administrative journeys, and document the ideal movement of data across the enterprise. Update the enterprise and information architectures to reflect the future state. Develop your roadmap.
- Evaluate your existing EHR, population health, analytics and/or integration vendor to see if they have a roadmap and strategy to meet your demands. Understand the specialty vendors in the market and track their evolution.
Business Impact: Successful deployment of a comprehensive health data convergence hub is a foundational component of the real-time health system, conducting digital healthcare, and the ability to execute population health and community care management. There is no question that how successful an HDO is in optimizing the use of its data has a strong correlation to achieving successful outcomes. The health data convergence hub facilitates the exchange of information and insight from origin to destination at the right time. In the U.S., continuing healthcare reform, including MACRA and MIPS, raises the stakes; globally, healthcare reform and e-health initiatives will also rely on more industrial-strength capabilities to share and exchange data.
Benefit Rating: Transformational
Market Penetration: Less than 1% of target audience
Maturity: Emerging
Sample Vendors: DataMotion Health; Halfpenny Technologies; Health Catalyst; Imat Solutions; Phemi
Health Value in Virtual Care
Analysis By: Bryan Cole
Definition: Health value in virtual care is the business model, technology integration, incentive design and messaging that, in combination, enable payers to obtain the highest financial, population health, analytic and consumer engagement benefit from a limited list of virtual health services that are in production today. This category includes only those technologies that a payer typically funds and implements, such as wearable health monitoring, and virtual or electronic physician visits.
Position and Adoption Speed Justification: Health value in virtual care is a new technology for payers on the 2017 Hype Cycle. While the category includes several discrete technologies, this profile tracks how payers have applied these technologies, integrated with other payer IT systems and implemented to orchestrate health value for members. Of the range of potential virtual care technologies, this profile focuses attention on tools that:
- Facilitate member access to care, such as on-demand virtual visits and e-visits.
- Aid payer care management efforts in areas like medication compliance management, wearable health monitoring and personal health management tools.
On-demand virtual visits are quite a common payer benefit today — often delivered through partnerships and at the behest of major employer group clients. The tools are poorly utilized by members, however, and often include high per-member, per-month fees that challenge the health-value proposition.
Better value will, instead, be achieved through integration and proactive application of virtual care to augment or replace face-to-face care interactions. Payer care management staff could potentially use the same technologies to lessen the burdens of routine patient health-status checking. Payer care managers could then use freed time for more valuable patient interactions, such as medication consultations or decision support, thereby reducing costs and increasing access. For members, access means greater convenience. Payers hope to improve care management, possibly preventing the progression of some diseases and lowering total costs. While members who use virtual care services are pleased, end-user adoption is still low. Barriers to broader payer adoption include:
- Cultural change and edification for more consumers to accept that virtual care can be as effective for some conditions
- Growing, but not complete, adoption of value-based payment arrangements that share financial gains when virtual care is championed by network providers
- Lack of payer medical policies on provider payment for virtual care and network provider contract terms
- Inconsistent state rules on providers giving care virtually
Consumer demand, better experiences, programmatic integration and improving technology will lead to mainstream payer adoption within the next five years.
User Advice: Virtual care to date has been very fragmented, with individual vendors each pursuing different technologies to address one element or another of patient health or member care management. For example, one vendor might have a remote cardiac monitor read by a physician in private practice, while another vendor offers a medication adherence program offered through the payer, with both installed in the same member's home. Thus, Gartner believes various stand-alone telemedicine solutions will be usurped by integrated telehealth platforms.
Consolidation of technologies and services from vendors meshes with payers' need for greater integration of virtual services to further their care management objectives. Payer CIOs actively support the trend of virtual care integration with care management by:
- Extending on-demand virtual visits and e-visits to any member segments without access to them today
- Expanding any existing pilot programs for wearables or in-home monitoring to additional member segments
- Integrating virtual care programs with quality improvement, risk adjustment optimization and care management IT systems
Business Impact: Many payers have isolated or pilot programs for virtual care in place now. Payers will obtain maximum health value for their members by expanding and integrating virtual care with care management programs. In the long term, increased access and earlier intercession, combined with effective incentives and metrics, will lead to improved member experience and health outcomes. However, there are trade-offs:
- Quality — There is emerging evidence that virtual care practitioners overprescribe antibiotics and are not as adept at diagnosing complex cases. Better practices and standards will evolve as adoption increases.
- Clinical data — Virtual care runs the risk of creating another silo of clinical data, unless payers utilize virtual care services staffed by network primary care providers or aggressively integrate data generated by virtual care practitioners.
- Short-term financial results — Emergency room and urgent care diversion is partially offset by increased member utilization of more convenient and lower-cost virtual services. Targeted promotion, smart incentives and value-based payments will refine the payer ROI of virtual care.
Benefit Rating: High
Market Penetration: 5% to 20% of target audience
Maturity: Early mainstream
Sample Vendors: American Well; Health Dialog; MDLive; Teladoc; virtuwell
Health-Value Product Design
Analysis By: Brad Holmes
Definition: Health-value product design is a composite profile that tracks payers' deployment of product components or end-to-end plan designs that make consumers' receipt of health value prominent in what is marketed, orchestrated, measured and reported. Health value is the measurable enhancement or maintenance of health status realized by individuals through their personal actions or engagement with the services, tools, products and content of the broad health ecosystem at an attractive price, with clear quality and with minimal personal disruption.
Position and Adoption Speed Justification: Given our focus on health value or the measurable impact on health status as the criteria for placement in the Hype Cycle, this configuration and deployment of payer product components, or total plan designs, is just emerging. Gartner first published its definition of this business model and category of plan designs in February 2017. We did so both as a vision for the future and also as a reflection of the conversion of customer demands and industry trends. End consumers, employers and government purchasers alike put increasing weight on care quality, satisfaction and health status restored or maintained as the results they want from their investment in health coverage. Payers and providers alike are taking more accountability for health results, not just unit costs or volumes. The logical end to this transformation, therefore, is a product (or prominent feature) that promises and reports health value results, not just the access, cost-sharing, club discounts, decision support, smiling babies and the like that typify payer's product marketing and performance reporting today.
Payers have to engineer a major transformation in order to deliver on the full health-value management (HVM) vision. Fundamentally, HVM is a digital business proposition and one that will only be credible as payers make the transition from analog to digital across all their basic business capabilities. However, that does not mean progress can't happen in the meantime. Hence, we expect to see increasing evidence of the health-value trend manifest in components of an overall product design and value proposition. For example, some payers today promote, measure, report and assume risk for the health outcomes of specific pop health programs. Others are orchestrating health-related services beyond traditional care. In addition, many are capturing detailed end-customer feedback on their personal health status to close the loop on their HVM promises.
Gartner's 2016 CIO survey reveals that payers' digital efforts were only half as mature as other industries in aggregate. The progression of health-value product design in this Hype Cycle is significantly tied to the digital business progress of the payers enabling and launching them. In the next five to 10 years, the convergence of payers' reorientation to end-user impact and overall digitalization will enable more health-value plan designs and product components.
User Advice: Payers have tended to define their value and core products on the basis of cost-sharing terms (co-pays), provider access (health maintenance organization [HMO], preferred provider organization [PPO]), spending support (health savings accounts [HSAs]) and wellness features (wearables and mobile apps). The transition to a new value story around end-customer health value received and perceived will take time. Organizations would be wise to take an incremental and progressive approach toward the new model by starting to capture member feedback on health status now and tracking change over time. Capturing that data is fundamental. CIOs of organizations moving toward this model must also engineer a more digitalized, open, adaptive approach to technology deployment as well as workflow, data, analytics and service collaboration with other organizations in the ecosystem of health. Health-value management (HVM) is a team sport.
Payers can take steps toward the model by focusing first on consumer engagement and population health management. Examples include payer partnerships with athletic shoemakers combined with wearable trackers, product discounts and community spaces to better satisfy the interests of health-conscious members. Other payers are focusing on intensive support from preconception through the first year of life to deliver palpably better health outcomes for mothers and their children while still others are rolling out remote monitoring to enhance the outcomes of homebound seniors. Component pilots like these help payers deliver, capture, report and promote the health value they orchestrate for a targeted group at a manageable scale. This kind of discrete pilot can be tried at the same time as longer lead time projects to modernize core systems, leverage the cloud, reinforce and invest in bimodal, and as innovation teams work their way through the organization and deliver a more digitalized platform for a full HVM model.
Another possibility is to build an independent business unit untethered to legacy systems in order to pilot a complete HVM product in partnership with a collaborative, progressive employer.
Business Impact: Health-value product components and plan designs have the potential to massively shift the business models of today's payers into something more valued by customers and profitable too. The advantage gained from earning trust, loyalty and increasing retention of end customers will eventually lead to a reshaping of the health insurance industry. Traditional payers will move to the commodity end of the value chain. HVM organizations will occupy the value-added, premium end of that spectrum. The middle ground will not be sustainable.
Benefit Rating: Transformational
Market Penetration: 1% to 5% of target audience
Maturity: Emerging
Sample Vendors: 23andMe; American Well; Apple; Emmi; Geneia; Medtronic; Optum; The Robotics Institute at Carnegie Mellon University; Zipari; Zocdoc
Precision Medicine
Analysis By: Vi Shaffer; Mark E. Gilbert
Definition: Precision medicine is an emerging approach for disease diagnosis, treatment and prevention that takes into account individual variability in genes, physiology, environmental exposures and lifestyle. In the context of this Hype Cycle, it combines advances in genomics medicine, wearables and the Internet of Things with enhanced data collection in electronic health record (EHR) systems, environmental sensors, wearables and mobile device applications.
Position and Adoption Speed Justification: Precision medicine, at its core, is linking patient observations from many domains with the prevalence of health and with the risk, prevention, onset, diagnosis and treatment of disease. It starts with a complete collection of data surrounding patient history, physical exam and routine laboratory studies. To those routine data elements, precision medicine adds genomic sequencing and microbiomic (skin, respiratory tract and intestinal bacteria) sampling to perform diagnosis and treatment. Over the next few years, precision medicine initiatives will collect real-world data (RWD) on patients' preferences, behavior (habits and lifestyle) and environment (what exposures to environmental agents, such as chemicals and radiation, patients may be having). It will take years to capture these RWD elements, standardize their recording and analysis and develop real-world evidence (RWE), correlating RWD with outcomes. Mobile phone applications and attached devices, wearable sensors, sensors and devices in the home and workplace, and publicly available data on the patients' environment will likely all be involved. Many of these technologies are in use today, but it will be more than 10 years before these levels of RWD and RWE are part of routine medical practice.
Healthcare industry use of the term "precision medicine" (PM) has been growing for some time. You can spot many vendors with "precision medicine" on their websites or in mission statements. PM is closely related to, but is a larger concept than, genomics medicine because it incorporates personalized knowledge about the patient beyond the molecular/clinical viewpoint. PM got a particular boost in the U.S. when former President Obama launched the Precision Medicine Initiative in 2015. In late 2016, Congress continued this direction with the 21st Century Cures Act. However, the amount of research funding focused on precision medicine in the 2018 budget is still an open question as significant cuts are in President Trump's first proposed version. HCA's Genospace, and Canadian startup Sequence Bio partnered to build a broad-scale government precision medicine initiative for Newfoundland and Labrador. Genomics companies are partnering with EHR vendors and integrated delivery networks: ActX with Epic, Allscripts with its 2bPrecise service line and NantHealth, Claritas Genomics with Cerner, Syapse with Intermountain Healthcare, Philips' cloud-based genomics platform with Illumina sequencing technology and BaseSpace Sequence Hub.
User Advice: Top executives, medical and service line leaders in life sciences, healthcare delivery and health insurance must all stay engaged with the advances under the precision medicine umbrella. Central to the precision medicine initiative is gradually collecting more detailed data about patients.
For CIOs, chief medical informatics officers (CMIOs) and other IT and clinical informatics leaders, precision medicine has a succession of IT needs for its support. Socialize and adopt a forward-looking healthcare analytics architecture. CIOs must lead the move toward the enterprise architecture, workflow/decision support design, and new partnerships that enable genomic analysis and recommendations for medication prescribing and cancer care. To advance your population health management efforts, CIOs may plan to engage a data broker or medical hub partner to collect and standardize clinical data from patient wearables and home devices. CIOs should include exploration of mobile applications for patients to collect chronic condition symptoms, medication effects and healthcare preferences. All of these platforms will ultimately be extended to capture the data needed and transformed into real-time use for precision medicine. Early experiences in cancer and certain chronic conditions will build the medical collaboration and competence for future precision medicine.
Business Impact: Between now and the decade-plus fulfillment of precision medicine's promise, there are ample opportunities for entrepreneurs; life science companies; academic medical centers; healthcare, health knowledge, cloud and decision support companies; EHRs and the like, to capitalize on its many emerging commercial tentacles. Precision medicine, based on RWE, reflective of the unique RWD of each patient, will replace evidence-based medicine based on a cohort of patients similar to the patient at hand. Artificial intelligence in healthcare will use precision medicine datasets across millions of patients to suggest diagnoses and treatments. This transformation should yield significantly reduced incidences of medical diagnosis error, reduction in treatment variability and ultimately reduced total cost of care. It should improve population health and further emphasize predictive and preventive actions. Precision medicine is needed to transform central medical decision making to personalized consumer engagement, which will drive the entire engine of healthcare delivery by 2030.
Benefit Rating: Transformational
Market Penetration: Less than 1% of target audience
Maturity: Embryonic
Sample Vendors: ActX; Allscripts; Claritas Genomics; HCA-Sarah Cannon (Genospace); Illumina; NantHealth; PathGroup; Philips; Quest Diagnostics; Syapse
Provider/Partner Alignment Solutions
Analysis By: Bryan Cole
Definition: Provider/Partner alignment solutions are the technology tools and services associated with managing the relationships of and interactions between payers, their contracted providers, and other partners in delivering health-value to members. These solutions integrate all of the data sharing, workflows, and contractual obligations necessary to support the full life cycle of provider relationships from network design and onboarding to claim payment, servicing, and contract renewal.
Position and Adoption Speed Justification: The provider network management applications technology profile has been renamed provider/partner alignment solutions to better reflect the IT and business process integration payers must undertake to collaborate with providers with a share focus on consumer outcomes under value-based payment and accountable care organization models.
Provider network management IT systems that help payers contract, credential, and load providers for claim payment are not new. These systems suffer from a lack of integration, inconsistent data formats, and poor usability. The result is data gaps, inconsistent provider directories, inaccurate claim payment, costly rework cycles, and poor member service.
Provider/Partner alignment is a new framework. It expands technology enablement beyond contracting, credentialing, and data loading to all interactions a payer has with its network of providers and partners. This capability allows payers and providers to collaborate to improve care outcomes and lower cost.
The technologies supporting provider/partner alignment are consequently immature. Pace of improvement is quickening, however. Several firms now offer provider network management solutions engineered to be the consolidated source of truth for provider data. Within two to five years vendors will enhance their solutions' functionality to support care management and quality improvement satisfying expanded alignment goals. In five to 10 years, a majority of payers will have applied this technology to their own operating environments.
User Advice: Payer CIOs must manage the increasing complexity of provider network relationships under value-based payment models as well as the increasing burden of provider data regulation. The applications and operations payer business teams have used for provider network management are mostly piecemeal and simply not up to this task. The answer is to envision all IT systems that support provider interactions in a holistic manner, with each component application a piece of an integrated ecosystem focused on increasing member health-value.
Gartner believes that by creating a comprehensive provider management discipline for healthcare payers, CIOs can maximize strategic investments while addressing the complexity of IT activities. Reliance on fragmented legacy applications and operational practices that are not integrated with other areas of the IT system must be modernized to a more integrated whole.
Solutions must address both the operational challenges of provider data as well as enable improved relationships with providers. CIOs and their executive peers can build trusted, mutually beneficial relationships with providers on the two key pillars of CRM and analytics.
CIOs should obtain support from business sponsors of legacy IT systems by assessing the costs of and risks arising from current practices. CIOs and their IT leaders must then create migration plans to purchase new common provider databases and retire the patchwork of legacy departmental or functional applications over time. Finally, CIOs must build data links and real-time integration to care management, quality improvement, risk adjustment optimization, and core administrative processing systems.
Business Impact: In an era of increased emphasis on care coordination and value-based networks, payer/provider relationships are a strategic asset for both organizations. For example, payers have a palpable need to bring products defined by network composition to purchasers. And provider need more comprehensive, ongoing relationships with their patients. Thus IT systems that help cultivate, support, and redefine those relationships play a strong role in both payers' and providers' digital transformation efforts.
The payoff for improving provider interaction application is not just about strategy, however, closing provider data gaps and making provider business processes more efficient will:
- Lower operating costs by eliminating duplicate entry processes and rework cycles.
- Improve provider data accuracy and consistency.
- Remove abrasion points for members seeking care.
- Smooth relationships with the providers payers depend up for health-value delivery.
- Speed claim payment, financial reconciliation, and audits with providers.
- Reduce the risk-of-state and federal regulatory penalties for poor provider data directory quality.
Benefit Rating: High
Market Penetration: 1% to 5% of target audience
Maturity: Emerging
Sample Vendors: Change Healthcare; Cognizant; Gaine; Newgen Software; Optum; San Tech
Product Configurators
Analysis By: Bryan Cole
Definition: Product configurators are IT systems composed of a database, workflows and document generation to manage the variability of payer health plans. For a healthcare payer, a product configurator typically replaces a heavily manual process scattered across various functions and lines of business with an enterprise system of record for all insurance products. Product configurators use rule sets to guide how payer salespeople, underwriters, product developers and operations teams accurately structure, price and administer plans.
Position and Adoption Speed Justification: Payers typically support thousands of product permutations encompassing cost sharing, benefit coverage and network variations. Product configurators help by managing the middle-office processes of plan construction for quoting, adjustment in the sales process, finalization for core loading and member document generation (for example, certificates of coverage or benefit summaries). Product configurators are especially useful in the large group commercial segment in which purchasers commonly demand custom cost-sharing combinations or specialized benefits designs.
Core administrative systems treat products as discrete stock-keeping units, and assign each an alphanumeric code within a hierarchical structure that ties that product code back to lines of business for provider network or medical code definitions. However, health benefit plans are also often approved by regulators in a manner that allows variability (such as any primary care copayment within the range of $0 to $50) with group purchasers demanding skinnier benefit combinations to lower premium costs.
Product configuration technology has significantly improved in usability and capability over predecessor document generation systems. Yet relatively few payers have replaced homegrown product IT systems or manual processes due to the immaturity of product configurator technology and the difficulty of tallying the indirect costs of current clunky operational workflows. In addition, some payers' inability to integrate product configurators with their legacy core administrative processing systems blunts the potential financial returns.
User Advice: To get the most from product configurator technology, CIOs should look for vendors that use:
- Web-based graphical user interfaces for ease of use, along with back-end open APIs for easier IT integration with underwriting, CRM and other applications that leverage product date to function
- Workflows and levels of user authority with boundary settings to approve simple (such as new primary care copay amount within approved range), medium difficulty (such as primary care copay amount outside of range currently filed with regulators) and significant (for example, exclude certain codes from primary care office visit set) product variations
Leading vended products also:
- Aid, but not necessarily automate, setup on core administrative system.
- Manage relationships between contract form numbers and product codes, especially as they change over time.
- Feed benefit data to more than just member documents, such as portals for members, providers and brokers, or required annual Affordable Care Act (ACA) benefit filings to Centers for Medicare and Medicaid Services (CMS).
- Integrate with premium rating engines and financial accounting tools to facilitate the processes by which actuaries, underwriters, informatics and finance personnel pull utilization data from data warehouses and core administrative processing systems.
- Support backward lookup from product codes on core systems to cost-sharing amounts and other benefits needed for custom care management and actuarial reporting.
Replacing outdated business processes is key to a successful product configurator installation. Business rules and staff roles around product configuration can grow haphazardly over time. Thus, CIOs must use the launch of a product configurator as an opportunity to document, audit and fix underlying process flows and decision loops. Business leaders must also partner with IT to set strong governance and user roles in place at the time of launch (for example, only underwriters can approve a benefit variation with premium impacts).
Business Impact: Product configurators offer:
- A far more organized and manageable product "shelf" for payer sales, product development/management, underwriting, operations and IT staff
- Automated production of member documents, such as a certificates of coverage or summary plan descriptions, ACA-mandated Summary of Benefits and Coverage, and unregulated benefit summaries
- Easier core administrative processing setup, ranging from standardized reports for product management, IT or operations staff to use when setting up new benefit packages to semiautomated setup via integration, depending on the core administrative system and product configurator being used
- Strategic visibility into product design, analytic enablement, and the ability to be more consultative with employer and government clients
- Improved compliance with benefit plan contract filings made with state and/or federal regulators
Staff and error rectification costs for current operations associated with this problem have been borne by product development, sales, operations and IT teams for years. Product configurators reduce these costs through:
- Administrative simplification and cost reduction — Streamlining middle-office processes so that downstream IT teams are involved only when finalized benefits must be set up on a legacy administrative system
- Improved compliance and error resolution — Controlling middle-office information and actions to avoid a sales or customer service representative quoting the wrong benefit, resulting in a member appeal
Benefit Rating: Moderate
Market Penetration: 1% to 5% of target audience
Maturity: Adolescent
Sample Vendors: FJA; HighRoads; Optum; Oracle; Pegasystems; The Most Group; ValueMomentum
AI for Healthcare Payers
Analysis By: Jeff Cribbs
Definition: Artificial intelligence (AI) is an IT system that can change behavior, without being explicitly programmed, based on collected data, usage analysis and other observations. Many applications of AI technology extend to healthcare payer functions.
Position and Adoption Speed Justification: This profile tracks the adoption of formal, enterprisewide AI strategies by U.S. healthcare payers. AI is rapidly gaining attention across all industries, and the U.S. healthcare payer industry is no exception. Efforts to date have generally been vendor co-development pilots, such as:
- Anthem's use of IBM Watson to streamline utilization management
- Healthcare payers' integration of AI capabilities from cross-industry technology providers (e.g., to enable chatbot technology in their member service centers)
Natural-language processing (NLP) applications use AI to simplify medical chart abstraction for risk adjustment or quality improvement. AI has also been used to accelerate pattern discovery in claims processing, though the subsequent automation is most often done with rule-based automation (like desktop macros or robotic process automation). Early results have been mixed, as expected. But, wherever AI pilots have worked, they have quickly accelerated enthusiasm for new applications and use cases.
Payer business and IT leaders are coming to realize that, for a technology category as disruptive as AI, opportunistic investments need to be coordinated by a larger strategy. This realization has led several to adopt a formal strategy for AI. This strategy has most often originated in an innovation center, or within another team explicitly dedicated to evaluating new technologies and trends. For the most part, these strategies have not yet transferred ownership to the senior executives who can bring them to pass. We expect that such strategies — socialized at the enterprise level and coordinated with AI-related business decisions — will reach mainstream adoption among payers in five years.
Representative vendors in this category do not offer "AI strategies" per se. However, at a minimum, they offer analytical, customized consulting services that cover AI strategy for at least three payer use cases.
User Advice: Every U.S. healthcare payer should have an explicit enterprise AI strategy. This strategy should be owned and maintained by a cross-functional team (sponsored by the innovation group, if it exists). The team should include IT, operations, medical management, sales and marketing, and informatics (or whatever domain owns the advanced analytics functions). Payers that have procurement or vendor management functions should include staff from those areas as well, since much of the AI strategy will be implemented in the context of vendor analysis and selection decisions. At this stage, the strategy does not need to be exhaustive. However, it should be a written document that is agreed-to by key internal stakeholders and that includes the following, at a minimum:
- How the enterprise will define AI
- How the enterprise views the impact of AI on the payer industry overall
- Where the enterprise sees the valuable use cases for AI
- How the enterprise will time its adoption of AI technology
- What criteria will be used to determine whether to build or buy AI capabilities
A key purpose of this document in the short term will be to manage stakeholder expectations about the state of the technology and to demystify hype and "AI washing" messages from vendors. (AI washing refers to adding AI language to products or services that have no material AI capabilities.) More sophisticated organizations with larger data resources are more likely to internally develop and deploy AI applications in the long term. The practical step toward this end today is to modernize the enterprise analytics architecture — especially the components of the data science workbench and the decision hub.
Business Impact: One of the key drivers for an enterprise AI strategy is the breadth and complexity of the potential AI use cases in the payer industry. Below are examples in each of five AI application categories:
- Virtual customer assistants — Health plan selection, medical shopping/digital concierge services, appeals and grievances
- Virtual personal assistants — Member self-triage, fitness and wellness coaching, medical scheduling, and navigation
- Smart advisors — Prior authorization and payment integrity
- Other NLP — Medical chart abstraction (for risk, quality or care management) and service center voice pattern diagnostics
- Smart IoT — Home health monitoring, and wellness app and device signal processing
Evidence of "lift" gained by AI approaches to these payer use cases is only beginning to emerge and is difficult to validate. We rate the business impact of having an AI strategy as high, recognizing that AI is very likely to, at a minimum, reduce administrative costs and optimize current revenue for those that effectively execute a strategy. AI certainly has the potential to be transformational to the payer industry, but we will wait for more concrete evidence.
Benefit Rating: High
Market Penetration: 1% to 5% of target audience
Maturity: Emerging
Sample Vendors: Fractal Analytics; IBM Watson Health; Scio Health Analytics
Member Engagement Hub
Analysis By: Jeff Cribbs; Bryan Cole
Definition: The member engagement hub (MEH) is a technology and process concept that ties multiple systems together to optimally engage the member. An MEH includes proactive and reactive communication, allows personalized, contextual engagement with members across all interaction channels, and orchestrates interactions across all payer functions. These capabilities enable synchronization of sales and marketing, member service, and medical management.
Position and Adoption Speed Justification: The MEH is the payer manifestation of the cross-industry customer engagement hub (CEH) concept. The MEH represents a generational, not an incremental, change to payer enterprise architecture, where the organization does more "personing" than processing. Whereas current payer enterprise architecture has largely been retrofitted to address growing member experience requirements, the MEH is purpose-built for optimizing every interaction with a member. The MEH is thus distinguished from current solutions by the material consolidation of member experience data, intelligence and data services into a single platform (or a handful of highly interoperable applications). Finally, the MEH connects with functional applications, such as core administration, care management and portal applications, to the extent needed to act as an orchestrator of them all.
Payers are moving incrementally toward MEH architecture with investments in these areas:
- CRM vendors, and the consulting firms that maintain a practice in integrating CRM products, are configuring tools specifically to support payer member experience requirements.
- Payer-specific member engagement technology solution vendors are expanding their capabilities down the application stack, from channel enablement to communications platforms. They are also expanding their scope from a single payer function to several payer functions.
- Payers are increasing investment in internally built applications that are intended to give various departments a "360-degree view" of a member's profile and interaction history with the enterprise.
- Payers are establishing more robust master data management for members and upgrading application interfaces with trusted data services.
It is unclear which of these early investments can be incrementally transitioned into a full MEH, and which will be replaced by new solutions as they appear across industries. As a result, we position MEH identically to the cross-industry CEH.
MEHs will almost certainly be a combination of internally built and externally bought applications, and because no single vendor offers a comprehensive solution today, representative vendors in this category offer key features aligned with an MEH.
User Advice: Most payer CIOs should maintain their current incremental investment in improving member engagement. The specific investments will vary based on which member journeys are important to the enterprise. Payer CIOs that seek to innovate specifically in the area of member engagement should ensure that their investments today are compatible with an engagement hub concept. This will, at times, mean forgoing quick wins with tactical solutions in certain engagement channels, in order to solve deeper architectural issues, including master data management and service-based application interfacing. Ensuring support from executive peers for these kinds of trade-offs through careful discussion, education and alliance building is essential.
Business Impact: In the context of Gartner's health-value management organization (HVMO) vision for the future of the payer industry, the MEH becomes the enabler of the last mile in the orchestration and delivery of health value to members. The MEH will deliver value to the payer business in the same way that the CEH will deliver value in other industries — with improved satisfaction, gained and retained members, and better brand advocacy. In the payer industry, however, additional sources of value can be realized in medical cost, operational efficiency, or revenue improvement via risk adjustment and quality-based reimbursement.
Benefit Rating: High
Market Penetration: 1% to 5% of target audience
Maturity: Emerging
Sample Vendors: Microsoft; Oracle; Salesforce; Teradata; Zipari
Modern Healthcare Analytics Architecture for Payers
Analysis By: Jeff Cribbs
Definition: Modern healthcare analytics architecture for payers refers to the next generation of enterprise analytics, as adopted by healthcare payers seeking to drive health value via pervasive analytical insight. Current payer analytics architecture often includes information portals (conventional reports and dashboards) and an analytics workbench (for data exploration). Modern architecture adds a data science laboratory (for advanced modeling) and a decision hub (to deploy insight into operations), and coordinates all four functional elements.
Position and Adoption Speed Justification: Most U.S. payers are more than a decade into their investments in classical BI and analytics architecture:
- Extraction, transformation and loading (ETL)-based data movement
- Enterprise data warehousing
- Reporting and dashboarding
- Data exploration tools
These investments have, by and large, performed well, as more payer business decisions are being informed by ever-improving analytical insight. In fact, many payers can still realize considerable value from classic BI architecture. However, the most innovative payers have started to experience the technical limitations of this architecture, and have begun to consider more modern approaches that could unlock new levels of health value.
Gartner research has defined the four functional components of modern BI and analytics architecture as it emerges across all industries. Of the 10 most important use cases for payer BI and analytics, the three that will drive adoption of modern architecture are consumer engagement analytics, population health management analytics, and provider/partner analytics. In each of these areas, leading payers have built or procured robust information portals and analytics workbenches, but generally possess limited data science and decision hub capabilities. No payers have these four functional areas working in a coordinated, comprehensive fashion for a business-critical use case. Rather, modernization efforts largely exist in PowerPoint decks, in skunkworks projects in innovation centers, or in early vendor pilots (for data lakes, advanced analytics platforms, or logical data warehousing, as examples).
Note that the positioning of this category is weighted by the size of the payer organizations adopting the approach and by the penetration of the approach within those organizations. Representative vendors in this category cover various components of the architecture. No one vendor encompasses all required capabilities or all payer use cases.
User Advice: All payer CIOs and data/analytics leaders should maintain their investments in classic BI and analytics architecture for the time being. New solutions will take years to stabilize to the point that they can replace the old ones, and even then, replacement will occur incrementally by function and use case. It is also likely that certain components of modern architecture, especially information portals, can be adapted from current tools to operate effectively in the new architecture. Investments made today in data governance and master data management will be almost completely transferable, and will position payers well as new tools, functions and use cases come on line.
For forward-leaning payers, data science workbenches and decision hubs are key areas for investment in data and analytics innovation. Even in the evaluation and pilot stages of an innovation project, however, CIOs should consider the path to assimilation in a modern architecture.
Later-adopting payers, as well as those that have determined these analytics capabilities won't be differentiating in the near term, should:
- Monitor the adoption of leaders.
- Wait for vendor offerings to become more robust and affordable.
- Re-evaluate annually for at least the next two years.
Business Impact: The adoption of modern BI and analytics architecture in the payer industry will be primarily driven by the challenges and opportunities of three use cases:
- Consumer engagement analytics — Payers are seeking to experiment with a vast array of consumer- and Internet of Things (IoT)-generated data in order to better understand and influence member behavior. Classic architecture cannot assimilate new sources quickly enough, and it cannot support the development of advanced behavioral models.
- Population health management analytics — As a starting point, payers need a more sophisticated analytical expression of health value — one that accounts for the interplay of cost, health and experience. With that understanding, they need pervasive analytics that are coordinated throughout the operations of the payer to drive that health value. Classical architecture limits both health-value modeling and coordinated, pervasive analytics.
- Provider/partner analytics — As the transaction processes of provider network management transform into the relationship management model of provider/partner alignment, payer analytics must be much more sophisticated in analyzing providers and the health value they can deliver to members.
Benefit Rating: High
Market Penetration: Less than 1% of target audience
Maturity: Emerging
Sample Vendors: IBM; SAS; Teradata
Community Resource Network Management
Analysis By: Jeff Cribbs
Definition: Community resource network management (CRNM) is an operational model that an entity (typically a payer, provider or government agency) adopts to optimize the utilization of nonmedical services by the individuals it serves. These resources are often delivered by nonprofit or government entities that address the social determinants of health. Key components of CRNM include:
- A directory of service providers
- The ability to refer individuals to service providers and track those individuals
- Analytics to assess the efficacy of service providers
Position and Adoption Speed Justification: Research studies and commentaries in leading health policy journals continue to conclude that the causal determinants of health (and, by extension, healthcare costs) are predominantly outside the healthcare system. If healthcare payers and providers are to impact these causal determinants, they need to extend their reach beyond the healthcare system and into the communities of their patients and members. One approach is to better coordinate efforts and, sometimes, payment with community resources like housing, healthy food providers, legal services, transportation services and education assistance.
Government grant makers, think tanks and thought-leading health policy foundations (especially the Robert Wood Johnson Foundation) are making grants to pilot and study care and payment models that better incorporate community resources. For example, in early 2017, the Centers for Medicare & Medicaid Services (CMS) Innovation Center awarded $157 million in funding through the Accountable Health Communities Model, which will "test whether increased awareness of and access to services addressing health-related social needs will impact total healthcare costs and improve health and quality of care." The Health Affairs journal recently published a study of 32 representative accountable care organizations (ACOs) in the U.S. The study found that half of these organizations have made concerted efforts to coordinate with nonmedical services (most commonly to address unmet needs for stable housing, transportation and food security) to support the new pay-for-value initiative. Population health thought leaders like Dr. Jeff Brenner at United Health Group and Dr. David Feinberg are driving such initiatives at their organizations and evangelizing the concept for others to follow suit. We therefore position CRNM prepeak in 2017. However, the evidence and enthusiasm represented by these pilot activities will drive CRNM beyond the peak quickly — likely in the next two years.
CRNM is the organizational competency that will be required to move these pilots to an enterprise scale. It will allow payer organizations to coordinate with and manage nonmedical service providers in a fashion similar to how they have managed medical providers for many years. It will allow providers to manage community resources in much the same way that they manage referral networks — in the context of value-based care. However, substantial challenges lie ahead in the following areas:
- Business — Aligning financial incentives, payment models and medical policy
- Technical — Addressing requirements for data quality and sharing, and for care management integration
- Cultural — Facilitating collaboration among clinical, social and technology workers from healthcare organizations, government agencies and nonprofit organizations
User Advice: We extend the following advice to both healthcare payer and healthcare provider CIOs:
- Drive the urgency of improving coordination with community resources by promoting CRNM with your population health peers. Invoke analogies from established, core competency "referral networks" or from "provider network management."
- Establish the business value of CRNM for your organization. Assign a business analyst to document the current state of community resource network integration within your organization. Identify use cases, user stories, pain points and opportunities for improved technology support.
- Form a cross-functional team of population health management (PHM) leaders and IT partners from your organization, and hold product demonstrations with at least one of the CRNM vendors included in this profile.
Business Impact: There is compelling emerging evidence that CRNM can deliver improved health at a lower cost. The largest, most persuasive studies are those that use CRNM in the context of value-based contracting. For example, in 2012, the state of Oregon initiated an ambitious delivery system reform for its Medicaid beneficiaries by creating 16 regionally based coordinated care organizations (CCOs). These CCOs receive a global budget for their attributed beneficiaries, and they have the flexibility to spend those funds on nonmedical services outside of the conventional guidelines of medical necessity. A 2017 Health Affairs study showed a 9% reduction in expenditures for the CCO population relative to a similar control. Studies of particular services (like educational classes for prediabetics or employment support for the mentally ill) and referral processes (like the CommunityRx program in Chicago, Illinois) put details around how such savings are realized. CRNM is labeled transformational for two reasons:
- The size of its impact on health and costs
- The extent to which it will require healthcare organizations to open themselves to coordination and collaboration with nonhealthcare organizations
Benefit Rating: Transformational
Market Penetration: 1% to 5% of target audience
Maturity: Emerging
Sample Vendors: Aunt Bertha; Healthify; NowPow; Purple Binder; Wholesome Wave
Member Health-Value From Wearables
Analysis By: Brad Holmes
Definition: Health value from wearables is a composite profile that tracks the delivery of health value that many wearable devices have been built and marketed to deliver and which payers use to justify subsidizing their cost for members. The devices in this category include both clinical and consumer-grade devices that span the more common smartwatches, wristbands and smart footwear to the emerging smart lenses, rings, garments and noninvasive glucose monitors.
Position and Adoption Speed Justification: Given our focus on health value from wearables or the measurable impact on health status, this class of technology in aggregate has largely disappointed to deliver on its promise. From the hopeful adoption by 32% of consumers globally for fitness trackers, yet disappointing retention rates, to equivocal impact findings for many devices and wearables, this class of technology is headed into the Trough of Disillusionment in our "Hype Cycle for Consumer Engagement With Healthcare and Wellness, 2017." However, the sensing technologies in wearables at the innovation trigger phase of our "Hype Cycle for Wearable Devices, 2017" continues to advance, e.g., perspiration analysis patches to monitor hydration or drug consumption and smart contact lenses to monitor ocular pressure or aid sight. As these sensing, supporting and dispensing technologies quickly improve, so too does the likelihood that consumer health value will follow.
The ultimate impact of wearables on health value is dependent, however, on the maturation of IoT, user experience, and AI platforms, which provide the infrastructure necessary for consumers to realize that value more easily, faster, and seamlessly. These link wearables to other services, data and algorithms that provide the personalization that a digitally connected wearable ultimately promises. Thus, health value from wearables is as dependent on the digital maturity of the ecosystem supporting the device as their native capability.
Gartner's 2016 CIO survey reveals that payers' digital efforts were only half as mature as other industries. In the next five to 10 years, the convergence of the next generation of wearables with payers' maturing digital capabilities will unleash greater member health value, placing this profile on the rise of the Hype Cycle.
User Advice: Payers have been cautious in their support of wearables. Gartner's research for enterprise CIOs looking to support wearables is decidedly conservative as well. Many of the vendors that are key to enterprise success with wearables are small players or startups with proprietary applications. Hence, we advise CIOs to conduct in-depth due diligence in picking partners and to adopt abbreviated lifespans for any devices supported in anticipation of rapid changes in capability. We also suggest that CIOs ensure business continuity by using traditional deployment and licensing models for wearables management tools.
Wearables' impact on health value won't happen in an isolated, device-centric way given the healthcare's complexities. Rather, picking a cohort of members inclined to technology adoption and aligning the incentives, data, multichannel support, analytics and user experience to match the health value objective desired is required. Gartner has predicted that payers will align with better-loved brands like Nike to take advantage of some members' natural affinity to that company as well as its established digital ecosystem for its exercise sensors, services and community. Tying those established capabilities to the payer's benefits, data, and related health services, and financing from health reimbursement arrangements (HRAs) and health savings accounts (HSAs) would have a multiplying effect on the health value received and perceived by that cohort. A runner could not only track her fitness changes, she could share them with her MD, be rewarded by her employer and use her HSA to pay for related care or allowable expenses.
High profile deals like the Aetna-Apple Watch one are newsworthy and exciting. Aetna's seeming commitment to the Apple ecosystem and the growing number of Apple Health apps give Aetna the option of becoming designed into the Apple product. However, the end results are yet to be realized and any path to delivering measurable health value will only be paved by connecting a rich ecosystem of health data, benefits, content, services and satisfying support to what is certainly a cool wearable device on its own. Without that ecosystem, many an Apple Watch will end up on the side table of well-intended wearable initiatives.
Business Impact: Wearables have the potential to deliver multiple valuable results for members, both on their own and as a channel for other services and sources of value. In this profile, we focus specifically on health value results for end consumers, which are considerable in their potential and breadth, from compliance for those with a chronic disease, to early detection and prevention or delay in disease onset, to wellness enhancement, to feelings of loyalty and satisfaction with the plan. Over the long haul, Gartner believes adoption will increase as both the devices themselves and the supporting digital ecosystems mature. The path to that result will be rocky, however, as is the case for most rapidly developing categories of technology. In the case of wearables, that rocky path is compounded by the many forms or sensing, delivery and integration of these devices with our many human systems that entrepreneurs are pursuing, let alone their connection to a digitalized business and ecosystem.
Benefit Rating: Moderate
Market Penetration: 5% to 20% of target audience
Maturity: Adolescent
Sample Vendors: adidas Group; Accenture (Chaotic Moon); Apple; Glucowise; Validic
Healthcare Consumer Insight as a Service
Analysis By: Jeff Cribbs
Definition: Healthcare consumer insight as a service (HCIaaS) refers to applications that:
- Source data from multiple sectors or industries.
- Employ advanced analytics techniques.
- Derive predictive or prescriptive health-related insight at the individual-consumer level.
- Deliver such insight into a workflow application via an API call.
Position and Adoption Speed Justification: Healthcare payers and providers are seeking efficient paths to derive more value from:
- Their own data
- Data from other sectors within healthcare
- Data from other industries
- Data from consumer interactions
The initial challenge is finding an efficient means of acquiring data, normalizing it to a multisector data model, and enhancing it through analytics. The next challenge is to:
- Derive the most valuable analytical insight (which is increasingly the realm of data science).
- Deploy that insight into the operational systems that need it (for example, the EHR, care management system, claims processing system or CRM).
This can be accomplished internally by modernizing the enterprise analytics architecture to include data science workbench and decision hub capabilities. However, the resource requirements of time, technology and expertise would put this out of reach for a majority of payers and providers in the near term. In recent years, HCIaaS has emerged to offer a faster, more efficient path to value.
Most HCIaaS efforts are in pilot or limited production stages at no more than a handful of clients. These implementations will be testing both the specific use cases of the insight and the delivery method. If and when there is demonstrable improvement over existing methods, the agility of the model will allow rapid market adoption by a larger number of organizations. We predict mainstream adoption in five years or less.
User Advice: Healthcare CIOs, IT leaders and analytics leaders should consider HCIaaS an emerging, and potentially crucial, component in developing their enterprise analytics strategy. The most promising use cases will be those that are experimental, that stand to gain the most lift from multisector data sources combined with advanced analytics techniques, and that can be delivered directly into a workflow application. For both payers and at-risk providers, analytics infused into the care management workflow application fits this description. Meet with your chief medical officer or your chief medical informatics officer to discuss the care management use case, and consider jointly attending an exploratory call with one of the representative vendors in this profile. If you are aggressively modernizing your enterprise analytics architecture, consider HCIaaS solutions as a stopgap to consumer insight solutions you may, someday, build and deliver internally.
Business Impact: HCIaaS offers a mechanism to gain the unique value of advanced analytics at the individual-consumer level, without the requirements of large datasets, on-premises integration of partner data sources, in-house data science talent, advanced analytics platform technology, and decision hub architecture for putting predictions into workflow. This type of service is especially important to small or midsize healthcare businesses, because it:
- Drastically lowers the barriers to entry for advanced analytics (including AI)
- Reduces the size requirement for many population health management use cases
- Allows for less risky, more agile solutions at this early stage of the technology
Early use cases for HCIaaS will be improvements of existing ones. For example, at-risk entities engaging in care management activities will replace their batch loads of "chase lists" and stratification scores — often generated from conventional licensed predictive models — with case-level API calls for consumer risk and stratification scores. The addition of consumer and sociodemographic data will provide better targeting and intervention strategies. Next, HCIaaS will bring advanced analytics predictions into the workflow for use cases that have high revenue impact, such as hospital readmissions for providers or underdocumentation of risk for payers.
Benefit Rating: Moderate
Market Penetration: 1% to 5% of target audience
Maturity: Emerging
Sample Vendors: CareSkore; Interpreta; Lumiata; NextHealth Technologies; VitreosHealth
BPaaS for Healthcare Payers
Analysis By: Bryan Cole
Definition: Business process as a service (BPaaS) is the delivery of business process outsourcing (BPO) services accessed via internet-based technologies and frequently sourced from the cloud. BPaaS services are often multitenant, automated, or have no dedicated labor pool per client. This technology profile tracks the overall adoption of BPaaS across both knowledge-intensive activities (e.g., utilization management, analytics and risk adjustment optimization,) as well as transaction-intensive ones (e.g., claims processing).
Position and Adoption Speed Justification: BPaaS is an emerging solution for healthcare payers. Payer adoption of BPO, or the delegation of business or IT processes to an external vendor, has gained momentum recently after years of slow adoption. BPaaS is not BPO, however, and payer adoption of cloud-based technologies still lags. For example, public cloud comprised just 0.6% of U.S. healthcare payers IT spending by category. Thus relatively few payers are taking advantage of the significant cost and efficiency gains possible when BPO is paired with cloud-based services.
Technology is not the limiting factor for healthcare payer adoption of BPaaS. Cloud-based offerings have become common in healthcare and routinely deliver secure, reliable results. Instead, BPaaS adoption is tied to broader payer BPO trends and payer recognition that outsourcing of any type can be an acceptable, secure, and reliable way to limit administrative costs.
Payers have looked to outsourcing most often to lower transaction costs for tasks such as claims data entry, document imaging and mailroom services, and billing. BPaaS, however, enables payers to also outsource higher value functions such as care management or expand quickly into new product lines like Medicare Advantage plans.
Note that positioning of this category is weighted by size of payer organization adopting the approach and the penetration of the approach within those organizations. Representative vendors in this category represent components of the architecture. No one vendor encompasses all required capabilities or all payer use cases.
User Advice: Healthcare payer CIOs should actively track the progress of BPaaS as a reasonable way to decrease their labor and technology footprint. Simply shifting complex business and IT processing to an outside vendor cannot solve existing cost or technology complexity issues, so CIOs must not assume that BPaaS will automatically improve their operations.
BPaaS must be the outsourcing of responsibilities as measured by results rather than simple tasks. Thus CIOs must put in place SLAs (covering both transactions and access) and tight operational and technology monitoring in place. Over time, these oversight functions must be routinized to ensure consistent, high-quality performance. Payers should also see BPaaS vendors as long-term partners, including risk-sharing, in order to increase accountability.
CIOs must review the value of transactional or single-service solutions against end-to-end strategic BPaaS options. Aggregated tactical solutions allow cost savings but not necessarily equal value across all payer business processes. Furthermore, strategic BPaaS can give payers access to high-value skills and a wider pool of in-demand resources allowing payers to expand in knowledge-intensive activities without adding significant internal staffing.
Finally, CIOs must prepare detailed risk management plans, including immediate, short-term and long-term mitigation plans, to minimize reputational and operational risk resulting from a BPaaS vendor disruption or subpar service.
Business Impact: BPaaS combines two discrete approaches in outsourcing and the cloud to help contain or reduce IT spending. BPaaS can also improve performance of business operations with specialized resources, enabling the organization to adopt new applications and deliver new value and services quickly and efficiently. Healthcare payer CIOs can address longstanding inefficiencies through external resources available through BPaaS.
BPaaS pricing models are consumption-based or subscription-based, making them ideal for calculating per member per month costs to budget commodity functions (e.g., claims adjudication or fee for service payment reconciliation). This model also lends itself to product line expansions or new ventures in which the payer does not have a strong internal knowledge base. An example here is a commercial payer entering Medicare Advantage for the first time that does not want to hire a team of government program specialists.
Benefit Rating: Moderate
Market Penetration: 1% to 5% of target audience
Maturity: Emerging
Sample Vendors: Cognizant; EXL; HM Health Solutions; Infosys; Nasco; Optum; Sutherland Global Services; Wipro
Consumer Journey Analytics in Healthcare
Analysis By: Jeff Cribbs; Mark E. Gilbert
Definition: Consumer journey analytics is the process of tracking and analyzing the way consumers use a combination of available channels to interact with an organization over time. It covers all channels the consumer has used, including those with human interaction (such as call centers or physician encounters), those that are fully automated (websites), those that provide assisted help to the consumer (live chat and co-browsing), those that are operated in physical locations (clinics) and those with limited two-way interaction (display advertising).
Position and Adoption Speed Justification:
In recent years, a number of tools and techniques for assessing and reimagining consumer experience have gained significant adoption in healthcare. These include persona development, voice of the customer and, in many cases, customer journey mapping. The output of these efforts among leading healthcare organizations has been beneficial to fostering an enterprise understanding of both the current and the target state of consumer experience. CIOs and their teams are doing serious work to meet the challenge of enabling these newly imagined healthcare journeys. This has created an urgent need to develop measurement capabilities that will give healthcare organization leaders feedback on the successes and failures of these journeys as they are enabled.
Relative to other industries, consumer journey analytics is just as promising in healthcare, but less mature and less adopted. This is largely due to the complexity of the journeys and channels in healthcare. A longitudinal understanding of consumer experience in healthcare must include in its scope important consumer touchpoints with:
- Other enterprises (e.g., doctors referring patients to external specialists for consults prior to a procedure)
- Other sectors (e.g., a patient checking out-of-pocket costs for a procedure)
- Other industries (e.g., a member earning wellness incentives through the use of a personal wearable device)
The prevailing practice of direct observation of interactions is not sufficient (e.g., call center monitoring). Healthcare analytics teams will need data from internal and external systems to make inferences and complete the picture.
Healthcare organization leaders will make progress in the next two years largely by limiting the scope of the journeys and channels they choose to analyze. The first digital channels that will be integrated and analyzed are those that authenticate and match users to master person identifiers employed in other enterprise systems (such as EDW, CRM/call center, claims processing and care management). Sources that require a more probabilistic approach are several years away. These include display advertising, marketing, using beacon technology in brick-and-mortar outlets, and tracking unauthenticated use across multiple digital channels.
User Advice: Healthcare CIOs, as well as leaders in IT, customer experience and analytics, should:
- Prioritize projects that analyze customer journeys across two or more channels over projects that continue investment in more granular analysis of single channels.
- Limit scope and maximize impact by choosing journeys that primarily leverage channels with authenticated users that can (ideally) be mapped to enterprise person identifiers. Alternatively, develop a plan to introduce authentication to the most relevant and beneficial channels.
- Use agile analytics approaches to quickly pilot customer journey analytics for important cohorts of customers. This pilot will give business and IT leaders a sense of what is possible, and will guide investment in building production capabilities.
Business Impact: Healthcare organizations stand to receive many of the benefits that other industries have begun to realize from customer journey analytics:
- Higher customer satisfaction from more seamless and personalized interactions across channels
- Increased visibility into the benefits that each interaction delivers to the overall journey, resulting in better investment allocation to support the overall relationship
- Better allocation of investment in functionality and capabilities for each engagement channel, to ensure the customer's needs are met at the earliest opportunity
- Refined, accurate consumer segments that increase the effectiveness of marketing campaigns
- More successful personalization tactics — whether on commerce sites, in communication channels or elsewhere in the customer experience — based on data that gives a more complete view of the customer's activity in multiple channels (instead of in a single channel)
In addition, healthcare organizations can obtain the following:
- Increased revenue streams tied directly to satisfaction measures (e.g., CAHPS), medical risk (e.g., risk adjustment) and channel utilization (e.g., patient portal adoption)
- A better understanding of how improvement in experience relates to improved clinical and financial outcomes
- A direct line of sight into how the following are either supporting or preventing the ideal customer journeys:
- Business partners within the sector (e.g., physician to physician)
- Business partners across sectors (e.g., retail clinics and payers providers)
- Business partners across industries
Benefit Rating: High
Market Penetration: Less than 1% of target audience
Maturity: Embryonic
Sample Vendors: Adobe; Alight Analytics; ClickFox; IBM; Nice; Salesforce; SAP; Teradata
Smart Health Plan Selector Tools
Analysis By: Bryan Cole
Definition: Smart health plan selector tools apply advanced analytics to large and diverse datasets to assist consumers in comparing and choosing a suitable health plan based on factors such as health risk, financial risk tolerance, current prescriptions and physicians, and experience preferences. Smart tools represent a significant advance in usefulness compared with simple plan selection tools (often embedded in private exchanges) that use consumer-selected, rule-based scoring to sort and filter health plans.
Position and Adoption Speed Justification: Smart health plan selector tools first caught payers' attention in line with the rising adoption of consumer-directed health plans (currently at 29% of commercial members per the Kaiser Family Foundation's 2016 Employer Health Benefits Survey). These tools support individuals in picking health plans that most closely align with their personal, financial, and health risk tolerance and goals. Payer interest in smarter tools subsequently grew, reflecting:
- Consumers' general lack of knowledge of health terminology, plan design and provider network types when choosing products on enrollment portals and public or private exchanges
- The growing number of health plan designs that individuals choose from on enrollment portals and private exchanges, making the decision process for individuals overwhelming
- Employers' interest in capping their benefit costs at a fixed level, which often leads to offering an expanded range of plan designs with an equally large range of cost and premium sharing options
Unfortunately, the business impact of smart health plan selector tools has been limited, stalling breakthrough developments in functionality or consumer benefits. Payers' reduction in the number of products available in the individual commercial market after 2016 slowed payer adoption of these tools as their focus shifted to profitability, as opposed to more consumer choice. We believe that a lack of payer interest has held back vendor development of smart plan selector tool technology. Most current health plan selection tools are not truly "smart," but rely on decision workflows and Excel worksheets to facilitate individual plan selection. This necessarily limits consumers' benefits, because plan selection guidance is not as personalized as possible. Furthermore, private exchange functionality includes basic plan comparisons, further reducing payers' sense of urgency.
We thus categorize current smart health plan selector tools as obsolete before the plateau in 2017. Our categorization could change for 2018, but tool functionality will need to be enhanced to meet the needs of a post-Affordable Healthcare Act (ACA) market, including the artificial intelligence capabilities that originally differentiated this technology. Tools must also expand to include plan network considerations and consumer medical shopping needs, given today's prevalence of both consumer-directed plan designs and value-based care networks. Finally, tools should work within the broader health ecosystem by recognizing that a complete solution for an individual may not be a single plan, but rather a combination of supplemental plans and noninsurance consumer services.
User Advice: Healthcare payer CIOs should understand that there are few vendors that actually apply smart technologies — the use of data analytics and algorithms — in their health plan selector tools. Most representative vendors we list largely aspire to, rather than deliver on, the smart objective. Thus, CIOs should look for vendors whose solutions can perform perceptual tasks, such as classifying large and variant data input streams in nonobvious ways to inform decision making at a greater depth than using only member-, payer-, provider- or employer-specific data. By combining health and financial data with behavioral, social, demographic and other nonhealth data, payers can expect to more closely align individual plan preferences with consumers' desired health outcomes.
Business Impact: Smart health plan selector tools help payers provide members with the means to pick an optimal health plan that addresses particular health and financial interests in a way that paper- or rule-based health plan selection tools cannot. By incorporating data analytics and algorithms into the plan selection process, payers can go beyond simple workflows, and lead members along an enrollment path that is more personal and results in a more suitable health plan match.
Benefit Rating: High
Market Penetration: Less than 1% of target audience
Maturity: Embryonic
Sample Vendors: ConnectedHealth; GetInsured; Obeo Health; Picwell
At the Peak
Generation 2 Medical Shopping
Analysis By: Jeff Cribbs
Definition: Generation 2 medical shopping is distinct from its predecessor in providing additional capabilities common to the digital-commerce experience in other industries. At a minimum, these additional capabilities must include:
- A comparison of nontraditional venues (such as virtual care, retail or workplace facilities)
- Connection with appointment scheduling and provider payment
- Improved coordination with adjacent parts of the consumer experience (such as self-triage, treatment decision support and medical banking)
Position and Adoption Speed Justification: In our 2016 Hype Cycle, we predicted that Generation 2 Medical Shopping will "face continued missteps and setbacks." As it happens, 2017 positioning reflects such setbacks. Tools internally built by large insurers have slowed in their development of new capabilities or have rolled back entirely from certain lines of business. Vendor solutions have postponed or canceled important implementations. Initiatives and resources that would enable development and adoption (such as innovation grant funding, policy research and new transparency legislation) have largely been focused elsewhere in the prior 12 months.
The individual components of a Generation 2 solution, which strive to replicate the kinds of experiences consumers have grown accustomed to in other industries, continue to show small signs of advancement (the only reason we nudge the positioning forward at all in 2017). Most leading Generation 1 vendors have, through partnerships, begun to list virtual care and retail alternatives to in-person office visits. The scheduling component has seen the following:
- Venture-capital-funded startups (for example, DocASAP)
- Improved API access to scheduling from electronic health records (EHRs) and practice management systems
- Heightened consumer expectations based on the scheduling capabilities available in consumer sites like Zocdoc
Still, broad adoption of this category relies on a level of ecosystem collaboration and data sharing that is extraordinarily rare in U.S. healthcare today. Until some sudden business impetus compels more rapid adoption, we continue to expect Generation 2 tools to reach mainstream toward the upper end of the five- to 10-year time frame.
Representative vendors in this space supply components of Generation 2 medical shopping; however, no single vendor can fulfill all of its requirements. A few of the Generation 1 vendors are developing toward Generation 2 capabilities, but for clarity, we do not include them in this profile.
User Advice: Payer CIOs and business leaders must agree on the strategic importance and prioritization of delivering a leading medical shopping experience to members:
- If enabling market-leading medical shopping is not among the highest priorities, CIOs should delay investments until easier, less-expensive solutions emerge, and competitive pressures force broader provider participation. CIOs should monitor:
- The results of early pilots
- The rate of provider participation (especially in opening scheduling APIs and posting reduced service pricing in exchange for prepayment)
- The advancement of vendor capabilities
- The capabilities of large payer competitors in the market.
- Those few who aggressively pursue Generation 2 in the near term will need to piece together vendor offerings for various components and devote significant development resources to coordinating the experience with other applications. Efforts to enable Generation 2 capabilities should be tightly coordinated with enterprise-level priorities in "consumer experience" and "digital strategy."
- Strategically, CIOs and business leaders must recognize that, when it is fully realized, Generation 2 medical shopping will substantially change the payer practice of provider network management. Those payers that are successful will derive the competitive advantages of being the first to market with these capabilities.
Business Impact: It is in a payer's interest to own and compete on a quality medical shopping experience, because the core of what members expect from payers is assistance in extracting value from the experience of healthcare and wellness. Generation 2 medical shopping is distinct from Generation 1 in its ability to deliver value beyond consumer selection of lower-cost care. These additional sources of value include a positive association of technology with the payer brand, improved member loyalty, better quality scores, reductions in administrative costs in the member call center and improved utilization of other population health management services offered to members.
Benefit Rating: Moderate
Market Penetration: 1% to 5% of target audience
Maturity: Emerging
Sample Vendors: DocASAP; PaySpan; PokitDok; SpendWell Health; Zocdoc
Genomics Medicine
Analysis By: Vi Shaffer
Definition: Genomics medicine and its IT support enables the translation of genomics into patient diagnosis, treatment, and personalized health/disease risk prediction and management. This includes genomics-specific data capture (family history) EHR workflows, testing and clinical decision support/knowledge management, data storage and analytics, and many fields, such as functional genomics, proteomics, epigenomics and pharmacogenomics.
Position and Adoption Speed Justification: Genomics medicine is one of the most important advances ever in medical science. Such an advance is as difficult to translate into beneficial practice as it is to uncover, and has required decades and extensive research to deliver. There are weighty barriers, including development and clinical trial and regulatory approval of new tests, drugs and therapies. It is equally challenging to make this knowledge actionable by physicians within their workflows (as well as for consumers). Experiences to date in oncology and across other disease areas are setting expectations high that genomics will solve many medical mysteries, driving substantial government and private research funding. Overall, however, and especially measuring against the opportunities beyond oncology, adoption is in the 1% to 5% range. However, there is substantial convergence on the technologies, test costs, decision support and processes for applying raw sequencing data.
These significant events are new signposts of increased momentum and the need for HDOs to solve the genomics delivery dilemma:
- The U.S. Food and Drug Administration's April 2017 announcement "allowed marketing of 23andMe personal genome service genetic health risk (GHR) tests for 10 diseases or conditions … the first direct to consumer (DTC) tests authorized for information to consumers on an individual's genetic predisposition to certain medical diseases or conditions."
- The Institute for Molecular Medicine Finland announced in 2016 it is building a platform that integrates genomic and health outcome data from Finnish national population biobanks into a globally unique and valuable big data repository.
- HCA, one of the world's largest health systems, in 2017 acquired Genospace to deploy its genomics decision support across its large-volume Sarah Cannon cancer services across the U.S. and the U.K.
- Geisinger Health System (U.S.) announced its "Springboard Healthy Scranton" program will prescribe healthy foods and sequence tens of thousands of citizens to study the genetic versus behavior origins of their high chronic disease prevalence.
In addition, for the longer term, Illumina, the largest maker of DNA sequencers, is launching a DNA sequencer with new architecture that it says "could push the cost of decoding a human genome from $1,000 to $100" — although that decrease will not come for years.
User Advice: Healthcare provider CIOs, CMIOs, and medical and population health leaders:
- Understand the evolving market. Become educated on different approaches and options.
- Plan for a rich combination of tools and knowledge/decision support services to incorporate genomics medicine in the disease domains they serve.
- Scrutinize EHR vendors for their plans to support genomics medicine needs, such as the ability to record, store, secure, and access genetic marker data from patients, and their ancestors and family members, within the individual patient's record.
- Understand that enhanced genomics decision support for diagnosis and treatment will likely come from a combination of traditional evidence-based content vendors, government sources, genomics data banks and bioinformatics providers.
- Plan to leverage FHIR for continuous connections between genomics and analytics results. Functional interoperability of this rapidly advancing knowledge with individual patient data in the EHR and clinician workflows will be critical.
Life science CIOs and IT leaders:
- Outline business process, compliance, regulatory and IT implications when including genomics medicine disciplines for decisions about research, therapies and business opportunities, while ensuring patient privacy.
Business Impact: The major value of genomics medicine so far has been in more finely tuned diagnosis and better-targeted cancer therapy and more careful prescribing for 120 or so medications. The use of genetics-directed chemotherapy is increasing. Prenatal care and genetic counseling are also active areas of value.
Long-term, the business and population health impact of genomics medicine will be substantial. Researchers, life science companies, healthcare providers, and consumers variously will require genomics raw sequencing data, analysis and recommendations from sequencing data, results integration with EHR system and therapy selection support. Information exchange is needed among scientists, providers, patients, and families for collaboration and counseling. Increasingly, medication prescribing will be based on the presence or absence of enzymes suggested by genetic testing. Disease diagnosis and advising patients on managing health risks will rely more and more on genetic analysis. New genetic markers are constantly being discovered, requiring frequent reanalysis of patients' sequencing data. In turn, EHRs will need to be always connected to genetic analytical results so that diagnosis and treatment decision support are accurate and timely. For genomics medicine to be practiced on a wider scale, sweeping changes to platforms accessed by healthcare payers and providers will be necessary to expose more analytical tools, which can be leveraged to design better therapies. It will also impact products under development at pharmaceutical companies, adverse event reporting and safety systems, and product development platforms.
Benefit Rating: Transformational
Market Penetration: 1% to 5% of target audience
Maturity: Emerging
Sample Vendors: 23andMe; ActX; Ancestry; Claritas Genomics; Eurofins Genomics; Illumina; NantHealth; Quest Diagnostics; Sarah Cannon/HCA (Genospace); Seven Bridges
Cloud for Healthcare Payers
Analysis By: Jeff Cribbs
Definition: Cloud computing is a style of computing that is both scalable and elastic. Vendors provide IT-related capabilities as a service to customers (such as healthcare payers). These capabilities are delivered via internet technologies.
Position and Adoption Speed Justification: This profile tracks the adoption of formal, enterprise cloud strategies by U.S. healthcare payers. Most payers deploy some applications in the cloud today. However, only a minority of these payers have adopted a formal cloud strategy at the enterprise level as part of the strategic transformation of IT. Key barriers to adoption are fading, namely:
- Security — It is increasingly clear that cloud deployments are just as secure as — and, in some cases, more secure than — on-premises deployments.
- Applicability — Countering executives' former belief that cloud was not appropriate for most payer organizations, industries and businesses of all forms, sizes and IT sophistication levels are benefiting from cloud technology.
- Priority — Competing priorities and lack of business clarity amid healthcare reform have given way to urgent initiatives to control costs and increase flexibility in payer IT shops.
Furthermore, cloud technology is foundational in supporting the most innovative ideas in the payer industry, including the health-value management business model. In addition, the elasticity and agility of the cloud facilitate digital member engagement (via mobile apps, the Internet of Things [IoT], wearables and portal integration). Collaborative technology platforms employed for multienterprise use cases will have better options for application interfacing if deployed in the cloud. (An example of such a platform is a population health management platform used by payers, providers and governments.) Cloud-based analytics environments offer the opportunity to spin up new instances of "big data" sandbox environments with reduced upfront investment and IT support.
As cloud for healthcare payers passes the peak, expect increased attention to challenges, delays and unexpected costs in cloud migration projects. Still, despite significant cultural and technical hurdles in executing the migration, Gartner expects the adoption of cloud to move quickly in 2017 as competitive and cost pressures mount, arriving at mainstream adoption in four or five years.
User Advice: Beginning in 2016, Gartner advised all healthcare payer CIOs to have an enterprise cloud adoption strategy. Of course, CIOs should not immediately begin migrating all workloads to public cloud deployments. Rather, each organization must create a cloud strategy that includes the decision criteria for what to migrate to the cloud and in what order. Generally, these criteria should increasingly favor cloud options sooner than later. Nonetheless, the decision will vary widely based on where the workload is in the application stack, what the business requirements of the use case are (e.g., data use restrictions), and how much control over the SLAs is needed.
Most solution spaces in the payer sector now include vendors that either are cloud-natives or have migrated to a true cloud deployment model. In general, net new development efforts and vendor engagements should be hosted in the cloud. All payer CIOs should articulate to the business an up-to-date position on public cloud, including its security, its appropriateness for the enterprise, its implications to existing data center investments, and its other benefits over on-premises solutions.
Business Impact: A cloud strategy is essential to optimizing the implementation, use and governance of cloud technology in a way that maximizes business value. This strategic approach stands in contrast to the reactive approach that most payer organizations have taken thus far, in which business-led acquisitions of cloud-based products have created uncoordinated and inefficient support demands on IT. A cloud strategy will support the drive toward a new IT operational model that will thrive in the emerging payer landscape.
Compared with on-premises solutions, cloud brings advantages in elasticity and agility. Although cloud technology can save costs, don't assume that the total cost of ownership will be lower in all payer use cases. Similarly, while public cloud providers will have more resources to defend against outside threats, the humans managing the cloud will continue to introduce vulnerabilities that CIOs must actively govern.
Benefit Rating: High
Market Penetration: 5% to 20% of target audience
Maturity: Adolescent
Sample Vendors: Amazon Web Services; Google; IBM; Microsoft (Azure)
Sliding Into the Trough
Retail Analytics for Healthcare Payers
Analysis By: Jeff Cribbs
Definition: Retail analytics for payers is the practice of enabling key customer-level measures of business outcomes that are mature in other retail industries, in the context of the highly complex health insurance business model. Examples include member lifetime value, member profitability, cost of sale, cost of support, likelihood of churn, win-back rate and next best action.
Position and Adoption Speed Justification: When the U.S. Congress passed the Affordable Care Act, it became clear that U.S. healthcare payers would need to adopt many of the business practices and technologies of direct-to-consumer industries. Analytics was no exception, and in the year immediately following the act's passage, interest in enabling key metrics spiked —especially in the retail industry. Through 2016, progress was very slow, primarily due to these barriers:
- Complexity of payer profitability — The factors that determine profitability are much more complex in the payer industry than in industries where retail analytics is most advanced.
- Lack of regulatory clarity — The complexity above is also subject to enduring legislative and regulatory uncertainty. This uncertainty has made it difficult to monitor and predict performance, even at an aggregate level, but especially at the member level.
- Siloed data and legacy IT systems — Extracting and integrating data from internal and external systems have been resource-prohibitive.
- Other investment priorities — Payer technology budgets have been consumed by more urgent needs, often relating to regulatory compliance, value-based payments and individual market instability.
The lack of adequate analytical insight has resulted in notable failures and missteps in the consumer-centric end of the healthcare market.
While some of these healthcare-specific barriers are becoming more manageable, the broader cross-industry trend toward intelligent, coordinated, digital interactions with customers is accelerating. This has reinvigorated the efforts by payers and the vendors who sell to them to enable retail analytics.
In 2017, adoption is uneven among the various metrics that make up retail analytics for healthcare payers. Retrospective measures that require only one or two data sources are relatively mature (member churn can be calculated from year-over-year enrollment files, and little else). Predictive measures that involve many data sources are rare. For example, member lifetime value requires:
- Consumer data
- Claims history (actual when available; imputed when not)
- Operational data on support costs
- Predictions on risk adjustment values
- Predicted compliance with revenue-related quality measures (like stars in the Medicare Advantage line of business)
In the vendor community, many have begun to adopt messaging and highlight product features in the language of retail analytics. Though they remain immature, efforts toward an enterprisewide "next best member action" have been substantial in the last 12 months, accounting for our decision to make a more advanced placement of the profile this year.
For the purposes of this Hype Cycle, we track retail analytics as an aggregate of the maturity of the underlying metrics, to assist clients in understanding the advancement of this important competency for healthcare payers. In this profile, a payer is considered to have adopted retail analytics when the metrics listed in the definition above appear pervasively in workflows across the enterprise, as they do in other direct-to-consumer industries. While we expect retail analytics to reach mainstream adoption in five years, the accuracy and sophistication of the metrics will continue to evolve well beyond that time frame.
User Advice: Payer CIOs, IT leaders and analytics/informatics leaders must take a bimodal approach to retail analytics. Mode 1 efforts should focus on enabling and deploying metrics that can be readily derived from a small number of high-quality data sources. Retrospective measures in these areas exist for most payers, but are often confined to the marketing department and need to be effectively deployed to operational areas. Relatively simple analytics tools and techniques can be utilized to build predictive models that anticipate these same metrics (predicting likely quality gaps rather than reporting past gaps, for example). Mode 2 efforts will require data science talent, new data sources of unclear value and quality, an agile development process, and, eventually, deployment through a decision hub. In their early iterations, these efforts may lack the precision and accuracy to drive operations — but, those that lead now, learn and adjust, will gain significant competitive advantage.
Business Impact: Retail analytics is an essential capability in enabling a healthcare payer to orchestrate member health value through intelligent operations. In an environment of increasing commoditization of payer functions, retail analytics may well prove to be the primary competitive differentiator between those who thrive and those who fail across markets. The business impact of payer retail analytics will initially be greatest in lines of business where annual, individual, multicarrier purchasing decisions are made — namely, the public marketplaces, the multicarrier private exchanges, Medicare Advantage and, in some cases, managed Medicaid.
Benefit Rating: High
Market Penetration: 1% to 5% of target audience
Maturity: Emerging
Sample Vendors: Affine Analytics; Genpact; NextHealth Technologies; Salesforce; Softheon; Zipari
Payment Integrity Solutions
Analysis By: Bryan Cole
Definition: Healthcare payment integrity systems and services enable claims to be processed accurately and reliably in a manner adherent to all applicable rulesets and with minimal revenue/payment leakage. To do so, these systems' functionality encompasses healthcare contracts and services, member eligibility, payment accountability, and exposure to fraud, waste, and abuse (FWA). The term is most often used to denote a program of sound payment practices and includes managing and addressing FWA.
Position and Adoption Speed Justification: Payment integrity solutions mitigate a broad range of potentially improper claims payment activities spanning revenue integrity, payment accuracy, payment recovery, as well as FWA prevention, detection and recovery solutions. Almost all payers have some form of payment integrity scanning in place today, although its use across lines of business and technology varies considerably.
The increase in real-time digital data exposes payers to more systemic payment integrity threats requiring more sophisticated payment integrity solutions. In response to market forces and payer demands, payment integrity solutions are broadening their capabilities to incorporate social analytics, predictive modeling, machine learning and contextual computing. Other capabilities propelling this technology profile forward include increased:
- Focus on relational data tools capable of linking together difficult-to-detect systemic causes of improper claims submissions and payments.
- Prevalence of pooled, cross-payer data analytics to uncover improper payment occurrences spanning a geographic region or within a specific group of payers that is experiencing similar threats or abuses.
- Number and variety of algorithms, including "smart algorithms" — algorithms that are capable of learning — that turn uncorrelated data into actionable insights.
- Interest in auditing solutions to identify inappropriate use of medications, as well as to support dental services and provider credentialing.
- Use of geospatial mapping of fraud to identify the likelihood of organized crime involvement that might go undetected otherwise.
Payment integrity technology and user adoption of it has advanced only incrementally during the past year. While top vendors continue to work on prospective detection and advanced algorithms, there have been no breakthroughs. Thus we have advanced this technology profile only slightly and for 2017 place it in the beginning stages of the Trough of Disillusionment.
User Advice: It is unrealistic for payers to expect to eliminate 100% of improper claim payments and related abusive behaviors. When improper payments do occur, a payment-integrity solution that offers in-depth market expertise, professional services, and smart software applications will result in optimal protection for payers.
Payer CIOs must implement payment integrity vendors whose solutions address improper payments, beginning before a claim is ever submitted for payment and continuing after — long after, if necessary — a claim has been improperly paid. In addition, payers should expect vendors to root out defective processes and shore up inexpert resources that are partly responsible for the occurrence FWA and add to payers' administrative costs.
Payers should also strive to reduce overpayments with increased detection and analysis. This includes a 360-degree view of member, provider, claims, relationships, and event data. Payment integrity solutions should also alleviate the payer's dependency on internal IT to solve payment integrity problems. Vendors can replace a payer's internally developed and poorly performing methods with simple-to-use solutions that provide end users with greater flexibility and decision-making capability. The combination of software tools, use of data and professional expertise provides the strongest protection against improper payments.
Finally, look for vendors that excel at both "detection and prevention" and "discovery and investigation" to provide full protection against improper pre and post claim payment risks and behaviors.
Most vendors offer a share of savings payment option which removes acquisition costs for payers. Vendors are also increasingly offering their services on second or even third pass basis. Combining these concepts means payers can leave their current vendors in place for a primary scan and then use a different vendor for a secondary scan of claims to find additional payment integrity opportunities. Gartner recommends this approach as a low-risk method to test vendor capabilities with the goal of eventual consolidation using a leading vendor.
Business Impact: Payment integrity solutions address the problem of improper payments across the payer's entire payment life cycle, beginning before a claim is submitted and following through after (in some cases, up to five years) a claim is paid. Vendors work closely with payer's provider network management and compliance teams tackling inaccurate provider, benefit and coding data, as well as deficient processes and inexpert staff. Payers with formal special investigative unit (SIU) resources may utilize the software applications and tools of a vendor to automate, monitor, manage, eliminate or recover improper payments, but choose to outsource analytical, investigative and legal services to the vendor's professional personnel. Payers can expect a 1% to 2% savings on claim expense for implementing a full-cycle payment integrity solution depending on current approach and willingness to disrupt some provider relationships.
Benefit Rating: High
Market Penetration: 20% to 50% of target audience
Maturity: Early mainstream
Sample Vendors: Change Healthcare; FraudLens; General Dynamics Information Technology; LaunchPoint; LexisNexis; McKesson; Optum; SAS; Truven Health Analytics; Verscend
Health Value From Self-Service Mobile Apps
Analysis By: Bryan Cole
Definition: Health value from payer self-service mobile apps is a payer's technology and business strategy to not just implement member-facing mobile services, but also integrate and expand them to deliver the highest possible health value. Self-service apps allow members to conveniently access their health services via a smartphone or tablet, and may also provide customer support via chat, Facetime or click-to-call features.
Position and Adoption Speed Justification: Gartner has renamed and refocused last year's self-service applications profile to better highlight the problem payers have in fully leveraging mobile technology to deliver on the promise of improving member health. For example, many payers have already implemented the basic functionality of member mobile apps. This includes an electronic member ID card, benefit coverage information (such as cost-sharing responsibility and accumulator data), provider directory and drug formulary search, claim status, access to health records, and health account balances. However, these apps — often disconnected from each other, as well as the internal IT systems used by payer staff to administer benefits — lag in end-user adoption and ultimately do not meet the high bar customers set for modern digital interactions.
In contrast, this technology profile highlights the ways in which payers can accelerate the adoption of next-generation mobile tools and integrate them to deliver new health value. A smartphone by itself is, after all, only a channel. Health value comes from tying two-way member communications to payer care management or member service actions using an underlying digital business infrastructure. In many cases, this will mean integration with an orchestration layer of member-centric CRM.
Payers have performance and design challenges to overcome if self-service mobile apps are to live up to their hype. Many payer self-service mobile apps contain incomplete or inaccurate data. It is not uncommon for a member to log in and find the payer has a member's old email address, is missing a member's preferred provider or displays latent member claims data. These gaps can alienate members from using self-service apps, and is a barrier payers need to address before consistent use and widespread adoption will occur. In addition, poor integration between front-end apps and back-end IT systems makes it difficult to provide a seamless experience for members using the customer support functions, such as click-to-chat. Thus, self-service mobile apps have passed the Peak of Inflated Expectations and are sliding toward the Trough of Disillusionment.
User Advice: Payer CIOs should work with business leaders to define strategic goals for member self-service mobile apps. CIOs can begin by identifying what self-service functionality is currently available to members and what health value members derive from each app. CIOs should next create a plan to build additional functionality with the highest health value. Examples of features that payers and members value include those that:
- Coordinate data, workflows and interactions across various payer business areas with providers and partners, such as visit scheduling, telehealth, wellness events, pharmacy refills and access to health accounts.
- Facilitate member plan selection, enrollment and premium payment.
- Enable easy-to-use navigation of plan features and real-time accumulated cost-sharing information.
- Allow for two-way communications to address service and appeal issues.
CIOs should seek a mobile platform or mobile app development partner to help harmonize multiple apps whenever possible. Members tend to economize the number of self-service mobile apps they prefer to use on a regular basis. Harmonizing distinct member self-service mobile apps increases the chance of remaining top of mind for members. Thus CIOs should:
- Provide consistency in mobile user interfaces with other member channels to deliver a predictable and easy-to-navigate mobile app.
- Design interoperability between the self-service mobile apps and business applications.
- Instrument the app to get real user analytics to guide what features to add next.
Finally, every mobile app added to a member's health ecosystem increases the number of interactions that payers, providers and health-related services have with members. Primary payer business areas that must work together to coordinate the design and delivery of self-service mobile apps are sales and marketing, member services, wellness, and care management. Payer IT areas that support distribution (communication, enrollment and payment systems), member services (CRM, care outreach and benefits administration), and data privacy and security must also align with business leaders to develop data management practices for the housing and allocation of information derived from and distributed through self-service mobile apps.
Business Impact: Well-designed, well-integrated mobile applications offer an opportunity for payers to fundamentally change their interactions with members and orchestrate new health value for all consumers. Immediate results are direct financial returns through reduced calls to customer service, as well as improved HealthCare Effectiveness Data and Information Set (HEDIS) quality scores and member health outcomes. However, the bigger gain is in long-term consumer engagement and population health management. Failing to coordinate the design and use of self-service mobile apps across the payer business areas and IT can result in missed opportunities for effective and satisfying coordination of care and customer engagement.
Benefit Rating: Moderate
Market Penetration: 20% to 50% of target audience
Maturity: Early mainstream
Sample Vendors: 3PHealth; Benefitalign; Diversinet; Kony; MicroStrategy; Newgen Software
Next-Generation Core Administrative Systems
Analysis By: Bryan Cole
Definition: Next-generation core administrative processing systems enable payers to manage their fundamental enrollment, premium billing, and claim payment operations in a more nimble and flexible manner than seen with older systems. Vendors achieve ease of payer employee use and lowered total cost of ownership by using service-based architectures for eased integration with other payer IT applications, rule-based configuration as opposed to custom code development, and increasingly cloud native or multitenant natures.
Position and Adoption Speed Justification: Core administration is not new. Next-generation core administrative systems, however, combine both core plus differentiating capabilities to form a suite of administrative applications that are configured to be more responsive to changes in payer strategies, regulatory requirements, and customer demands. Capabilities include membership management, premium calculation, application of network pricing to claims, application of member benefits to claims, maintenance of member benefits and plans, and provider payment. Modules group capabilities by specific processes such as enrolling members, processing premium payments, maintaining benefit plans and provider contracts, adjudicating claims, and generating reports.
Technology for next-generation core administration is well proven, so impediments to mainstream adoption are based on business priorities and costs. Payer CEOs, CFOs, and CIOs have heard too many horror stories of core administration system replacement projects gone awry but the rationale to improve underlying technology capability and lower transactional costs when compared to legacy systems is still strong. Thus next-generation core administrative systems vendors must help drive wider adoption by lowering installation costs and risks for payers while providing timely functionality updates to meet changing market and regulatory demands.
Since next-generation core administration systems process purchaser premium payments received and provider claim payments remitted, we have consolidated the automated premium billing and automated provider payment technology profiles into the next-generation core administrative systems profile this year.
User Advice: Next-generation core administrative processing systems must enable payers to nimbly meet changing market demands, regulatory requirements, strategic priorities, and competitive pressures. A key distinction between next-generation and current core administrative systems is how well they integrate with associated IT systems. CIOs should thus:
- Offer a vision to business leaders of how a modern system will make it possible to expand capacity and capability to deliver both cost savings and new revenue streams.
- Install IT systems that address compliance and regulatory mandates, service new lines of business, expand member engagement, increase care coordination, enable new product designs, and support new provider contract arrangements.
- Choose vendors whose approach best supports the organization in transforming IT and the business environment. Vendors are increasingly specializing to support specific lines of business, types of users and technology trends. CIOs must carefully consider whether specialization is needed and if the vendor is focused on the same business priorities as the payer.
- Look for next-generation core administrative solutions that offer modular components, which can be easily integrated with existing administrative applications and can be readily expanded to incorporate new payer business models and value propositions.
- Consider whether licensed applications, SaaS, or business process outsourcing (BPO) solutions will best fit the organization's future-state technology roadmap. All next-generation core administrative vendors offer SaaS or cloud-based solutions in response to the growing "as a service" economy and pricing models. In fact, many no longer offer on-premises applications. These "pay as you go" systems make it possible for payers to define and redefine rent arrangements as their needs or business models evolve.
Business Impact: Core administration is a business-critical function for payers. As the "source of truth" (or system of record in Gartner's pace-layered application strategy terminology) for data next-generation core administrative systems offer high business benefits of lowered transaction costs and the ability to focus IT resources on applications closer to the customer that support innovation and market differentiation.
Next-generation vendors are focused on emerging industry trends such as consumerism and value-based payment arrangements. These and other disruptors require agility, use of real-time data analytics, robotic process automation, machine learning, and algorithmic processes. Vendors deliver solutions as modular applications or components that can integrate with payer or third-party applications using APIs and business process management. In this way, next-generation systems create more seamless and coordinated services and a more holistic solution than legacy core administration.
Benefit Rating: Moderate
Market Penetration: 5% to 20% of target audience
Maturity: Early mainstream
Sample Vendors: HealthAxis Group; HealthEdge; Invidasys; Virtual Benefits Administrator (VBA); Wonderbox Technologies
Clinical Data Integration
Analysis By: Jeff Cribbs
Definition: Clinical data integration for payers is the acquisition of patient clinical data from an electronic health record (EHR) system or health information exchange (HIE), and the integration of that data with payer-owned systems and business processes.
Position and Adoption Speed Justification: Clinical data integration (CDI) is an urgent issue for U.S. healthcare payers in 2017, garnering the attention of payer CEOs, government policymakers, and health information technology (HIT) vendors. The state of CDI today is highly fragmented as payers don't typically acquire and process with any consistency. Collection mechanisms vary by use case, line of business, provider type, and the payer's degree of digitization and automation. No payer today manages and analyzes clinical data with an efficiency and thoroughness comparable to, say, claims data.
The cultural and business alignment challenges between payers and providers have been a substantial barrier to progress. In several cases, payers have made significant investments in building a medical records repository, point-to-point connectors to particular EHR instances and provider portals for document submission (for clinical audits or prior authorization, for example) — only to find the vast majority of providers ultimately unmotivated to participate in data sharing. Fingers point in both directions when these projects don't deliver — but ultimately solutions are found when the financial incentives are aligned.
Technical challenges are waning, but remain substantial. More consistent use of interoperability standards among EHR vendors and a series of products and partnerships among payer and provider technology vendors point to more plausible technical solutions. As a result, most U.S. payer organizations today have acquired some amount of structured, machine-readable, clinical data, most often in message formats (such as an HL7 Continuity of Care Document [CCD]). However, for this data to deliver value, after the payer acquires clinical data, it must be normalized and integrated into operational systems. Recently, it is most often the failure of CDI projects to deliver on these last two steps that have frustrated business and IT stakeholders and driven CDI to the trough in 2017.
The most efficient technical solution for long-term acquisition, governance and use of EHR-derived clinical data is to acquire the data once; parse, cleanse and atomize it in a common normalization process; store it in a secure, relational medical records repository; and serve it up to the application layer to support its many use cases. However, the most reliable way to actually acquire clinical data is to engage a number of vendors to "chart chase" separately, using semiautomated retrieval at best (and more often, phone calls, fax machines and office visits). Gartner research indicates that adoption in the next two years will be dominated by the latter, tactical solutions. Efficient, enterprisewide solutions will emerge in the three- to seven-year time frame. For the purposes of tracking on the Hype Cycle, either approach qualifies as payer adoption of clinical data integration, based on the definition of this profile.
User Advice: Payer CIOs should prioritize their clinical data integration efforts first by assessing the degree to which data sharing is financially beneficial to both the payer and provider organizations (often included in value-based contracting terms). Where there is substantial business and cultural alignment, embrace a multipronged approach to clinical data integration in the short term (two years), focusing on the most urgent use cases (risk score accuracy and quality measurement). Thoroughly substantiate any claims made by vendors regarding capabilities in clinical data exchange. Begin to plan, if not yet invest in, a consolidated, enterprisewide solution. In planning, be sure to place sufficient emphasis on normalization and integration of clinical data, not just the acquisition of the data.
Business Impact: The acquisition of clinical data is a critical capability for U.S. healthcare payers with high, near-term business impact. The two most urgent use cases from a payer perspective are:
- Risk Score Optimization — Increasing documentation of medical risk such that it is accounted for in the risk adjustment mechanisms of certain lines of business such as the Hierarchical Condition Categories (HCCs) submission in Medicare Advantage and public exchanges.
- Quality Measurement — Improving the Healthcare Effectiveness Data and Information Set (HEDIS) and Medicare stars measures by supplementing administrative data with data from EHRs.
These use cases have a direct, large, short-term impact on revenue in the fastest-growing lines of business in the payer industry. CDI will deliver value to payers in two ways: (1) by increasing the "lift" of supplemental clinical data by acquiring more data and more complete data, and by extracting more meaning from that data; and (2) by decreasing the administrative, often manual, burden of acquiring and interpreting clinical data.
Benefit Rating: High
Market Penetration: 5% to 20% of target audience
Maturity: Adolescent
Sample Vendors: Availity; Halfpenny Technologies; Inovalon; InterSystems; MedeAnalytics; Orion Health; Post-n-Track; Redox
Climbing the Slope
Member Incentives for Wellness
Analysis By: Jeff Cribbs
Definition: Member incentives for wellness are the techniques used to encourage wellness among healthcare plan members by providing direct monetary benefits such as reduced employee contributions to premiums or additional contributions to a health savings account. Incentives can be tied to participation in wellness programs (such as attending a webinar or speaking with a health coach) or to verifiable wellness outcomes (such as achieving biometric thresholds or physical activity levels).
Position and Adoption Speed Justification: Our placement of member incentives for wellness reflects a combination of the prevalence of the practice (relative to total insured membership) and the size of the incentives being used (relative to the maximum allowed by law). Under the U.S. Affordable Care Act (ACA), an employer may offer monetary incentives up to 30% of the overall cost of the policy to promote participation in wellness programs and the achievement of wellness outcomes. For these amounts to be put in perspective, in 2015, an employee who achieved compliance could save about $1,931 on an employee-only policy, or $5,443 on a family policy, relative to his or her noncompliant peers (using average 2016 policy costs). Surveys indicate that a growing number of employers use these types of wellness incentives today. It is most prevalent among large employers, where over 35% provide financial incentives for completing health assessments, completing biometric screenings or participating in wellness programs. Those that do, generally keep the monetary amounts far below the levels allowed by current legislation.
Adoption has advanced incrementally over the last year — as more employers use larger member incentives for wellness as an alternative to blanket increases in cost sharing as premiums rise. Notably in 2017, we have decreased our Time to Plateau, and we now expect the category to reach mainstream adoption in less than two years. This first reflects the reduction in uncertainty regarding the legal status of these incentives. Several important cases have been decided in the past two years that have the net effect of assuring employers who advance incentive programs that they will not fall afoul of the Equal Employment Opportunity Commission (EEOC) — all of which were pended or decided in the employer's favor. In addition, the new federal leadership has made it clear the member incentives for wellness will not be rolled back. Paul Ryan's "A Better Way for Healthcare," for example, commits to "back wellness programs" and ensure that "employers are able to reward employees for making healthy choices." The same line of thinking around personal responsibility may result in the expansion of member incentives for wellness into government-sponsored lines of business. Our 2017 payer prediction anticipates this trend: "By 2020, three states will save 5% of Medicaid capitation spend by requiring beneficiaries to use a web-enabled health engagement tool." Taken together, these trends suggest member incentives for wellness will graduate the Hype Cycle in less than two years.
User Advice: Member incentives for wellness have the potential to benefit plan sponsors, members and innovative payers. Payer business and IT leaders should adopt an approach with clients that is flexible and consultative. On one hand, they must ensure they have the technology and services in place to support a wide range of requirements for wellness programs and value-based plan designs, as plan sponsors think creatively to design incentives tailored to the unique needs of their membership. On the other hand, they must be intentional about analyzing these incentives, establishing best practices, learning quickly from both successes and failures, and presenting these findings to clients. In many cases, the payer brand will be as exposed as the employer's brand when these incentives are introduced. Thus, it is essential that both parties avoid the perception and reality of nefarious motives or incompetent execution.
Business Impact: Member incentives for wellness are often positioned as mechanisms to improve population health or generate sustained member engagement with a one-time financial reward. The evidence on those two points is inconclusive, at best. However, payers that wish to build a brand around concepts of wellness, personal choice, empowerment and shared accountability can use wellness incentives to put actual financial incentives behind these themes. In government-sponsored lines of business, it would logically follow that providing financial incentives for certain behaviors could be used to improve quality measures and close coding gaps for improved risk adjustment, but very little evidence is available to support or refute this potential value. While it is true that many legal questions have been settled in favor of the practice, these incentives will continue to be controversial. Some see these practices as a fairer, merit-based way to distribute medical costs; others see them as ineffective, an infringement on privacy or, worse still, a means of discrimination. Payers that lead in bringing these offerings to market will undoubtedly find themselves in some amount of controversy, and will need to clearly and transparently communicate the opportunities, safeguards and success stories of their programs.
Benefit Rating: Moderate
Market Penetration: 5% to 20% of target audience
Maturity: Early mainstream
Sample Vendors: NovuHealth; Sharecare; Virgin Pulse; Vitality; Welltok
Generation 1 Medical Shopping Transparency Tools
Analysis By: Jeff Cribbs
Definition: Medical shopping transparency tools are applications that support the consumer practice of considering two or more alternatives for receiving a certain medical service. They provide comparisons of price at a minimum, but may also include measures of quality, convenience and consumer satisfaction. This is in contrast to the historical practice of obtaining services from the single provider or facility that was suggested by the health plan, referring providers or others (such as family or friends) without considering alternatives.
Position and Adoption Speed Justification: Medical shopping transparency tools are ascending from Trough of Disillusionment in 2017, as payers adjust their expectations of this generation of technology and find incrementally improving consumer adoption. While payers continue to express ongoing dissatisfaction with the capabilities and execution of the current vendor landscape, the data exchange challenges and worst functional gaps (like real-time integration with benefits accumulator data) have been significantly abated. Publicly available tools hosted by states, foundations, or the Centers for Medicare & Medicaid Services (CMS) itself are symbolically important, but effectively unusable to consumers. Where there is advancement in adoption of these tools, it is driven by these factors:
- An increased percentage of membership with the financial incentive to shop. After three consecutive years with near-zero growth, high-deductible health plans (HDHPs) reached 29% adoption among employees in 2016. Greater than 51% of members insured through their employers have annual deductibles of more than $1,000.
- Ongoing regulatory requirements for price transparency, often driven by state level legislation.
- Integration with call centers, care management or, in its fullest realization, payer "medical concierge" services.
User Advice: Healthcare payer CIOs and technology leaders who must deliver on medical shopping requirements in the near term should communicate the limitations of current-generation medical shopping products to business stakeholders, and act efficiently and decisively to meet minimum business requirements. In the midterm and long term, connect strategic planning around medical shopping transparency to business efforts in consumer experience transformation, often found in marketing or in a cross functional workgroup.
Convene a solution team to analyze next-generation medical shopping transparency capabilities and gaps between current capabilities, and design a high-level architecture and application portfolio that closes these gaps.
Payer CIOs selecting a medical shopping transparency vendor should prioritize open architectures and a clear vision on the convergence of medical shopping with other components of consumer navigation of healthcare. This includes enrollment, wellness programs, medical banking, incentive management, self-triage and treatment decision support.
Business Impact: Exposing consumers to the cost of healthcare services can, in some cases, accomplish what many other current health initiatives cannot — removing medical costs from the system. Consumers with high deductibles can immediately realize the savings of choosing a lower-cost option. In the long term, medical shopping tools, with a cohesive consumer experience, will enable new value streams. These streams include open-network provider bidding, increased utilization of telemedicine, reduced administrative expenses and a positive consumer association of technology with the payer brand. Because the tools include other comparison points — such as quality, satisfaction and experience measures — consumers will also gain the engagement that comes with informed choice. In the short term, however, the lack of consumer adoption and limitations of this generation of tools sharply limits this value, resulting in the low benefit rating.
Benefit Rating: Low
Market Penetration: 20% to 50% of target audience
Maturity: Early mainstream
Sample Vendors: Castlight Health; Change Healthcare; ClearCost Health; Compass Professional Health Services; Healthcare Bluebook; HealthSparq
Private Exchange Technology
Analysis By: Bryan Cole
Definition: Private exchange technology provides a self-service, web-based portal solution through which employers, employees or individuals can shop for, enroll in and pay for a health plan (and related products and services) from a single health insurance carrier. Self-service tools personalize the plan selection process. Private exchange technology must support a single carrier (i.e., payer hosted) but may also support a multicarrier (i.e., broker hosted) private exchange.
Position and Adoption Speed Justification: The market for private exchange technologies for U.S. healthcare payers is evolving in response to:
- Affordable Care Act (ACA) stipulations under which payers rely on private exchanges to integrate with public exchanges, as well as to enable brokers to enroll new members outside public exchanges as web based entities as defined by ACA regulations.
- Possible ACA replacement policies which emphasize direct to consumer sales on payers' own websites.
- Online broker-run enrollment solutions that offer health plans and related products from multiple payers and threaten to commoditize payers' brands and erode margins.
- Digital commerce sites in other verticals that have increased consumers' expectations for richer, more-efficient customer experiences.
For 2017, we are lowering the benefit rating of this technology to reflect limited employer adoption of defined contribution models along with payer implementations that have not revolutionized direct to consumer sales. The technology is reaching mainstream adoption, with only incremental evolution in the past two years.
User Advice: Payers that launched private exchanges in anticipation of the Affordable Care Act's 2014 market faced challenges of high implementation costs, unexpected integration complexity, and relatively low end-user adoption. To best address these concerns, CIOs should look for private exchange vendors that provide:
- Strong CRM capabilities for lead generation and customer acquisition, and for workflow integration with downstream care management or large group underwriting applications.
- Fully automated plan selection, payment and fulfillment capabilities to increase ease of use and minimize the need for payer support staff.
- Ease of integration with other payer IT applications, as well as with HIXs and third-party applications, to avoid manual workflows between systems and improve data sharing.
- Administrative portals and support tools for use by suppliers and channel partners to increase market reach, and expand product and service offerings.
- Rich use of data to support user decision making, generate reports on product selection and payment behaviors, and assess members' predilections when enrolling via the platform.
CIOs should also assess how the vendor's private exchange solution will lower administrative costs and increase per-member ROI. CIOs should thus consider vendors that:
- Are proficient in supporting multiple lines of business (LOBs).
- Streamline the sales process and eliminate excess workflows and manual processes.
- Provide cross-sell and upsell recommendation engines.
- Support a wide variety of health, wealth and ancillary products.
- Understand the regulatory and compliance requirements associated with the membership being served through their solution.
Finally, payer CIOs should exercise extreme caution when purchasing a private exchange expressly for the individual medical segment. Various ACA replacement policies under discussion by CMS as regulation and working their way through the U.S. Congress could dramatically change payers' requirements for individual segment private exchange technology. Thus, with a reduced benefit rating in group business and unclear regulatory environment for individual lines, CIOs must emphasize customer journeys, member ease of use, and analytic support when justifying private exchange purchase this year.
Business Impact: CIOs, IT leaders, and sales and marketing executives who own the administrative process of enrolling new members all have a stake in this technology. These leaders are seeking to streamline and enhance the shopping, enrollment, payment and onboarding processes of their members, groups, and brokers.
CIOs are also looking across their administrative operations for redundant or siloed applications that, if consolidated, would lower the cost of ownership and streamline disparate applications and IT resources. CIOs can expect the implementation of private exchange capabilities to support their application rationalization efforts.
The most common business lines that private exchanges support are small groups (whose employees may be eligible for a qualified health plan that can only be purchased through a public exchange) and individual consumers, along with the brokers supporting these two member populations. However, use with Medicare Advantage products and in retiree groups is expanding.
Benefit Rating: Moderate
Market Penetration: 20% to 50% of target audience
Maturity: Early mainstream
Sample Vendors: Benefitfocus; Colibrium; ConnectedHealth; Connecture; Empyrean Benefit Solutions (Bloom); GetInsured (Array Health);
HealthPlan Services; Online Insight; Softheon; Vue Software
Entering the Plateau
Risk Adjustment Management Systems
Analysis By: Bryan Cole
Definition: Payer risk adjustment optimization systems identify and prioritize member claim records with potential underreporting of condition severity or the omission of additional conditions. Many also track cases and schedule provider visits for members as part of a coding gap closure campaign. Complete risk adjustment management systems include — or are assembled from components by integrating — analytics, case management, and reporting to government agencies, major commercial group purchasers or providers paid on a value basis.
Position and Adoption Speed Justification: Payer risk adjustment optimization systems identify and prioritize member claim records with potential coding errors or omissions for further inspection. Most also track cases and schedule chart review visits for auditors as part of a coding gap closure workflow. Complete risk adjustment management systems include analytics, case management and reporting to optimize revenue from government or private sources.
Virtually all Medicare Advantage payers have a risk adjustment optimization program. These efforts run the gamut, however, from simple medical record tracking and desktop reviews through very sophisticated vended solutions that apply a combination of advanced analytics, artificial intelligence and clinical medical record reviews. Gartner positions risk adjustment management systems on the Hype Cycle based on the state of current solutions:
- Scope — Deployment of complete IT system capabilities and the application of shared processes in support of managed Medicaid, the Affordable Care Act (ACA) and other risk-adjusted business lines, along with provider and regulatory reporting.
- Capability — Use of learning algorithms, natural-language processing and artificial intelligence technology to make risk adjustment management systems more effective at finding member cases with medical coding gaps, as well as more efficient in obtaining clinical information to support revised coding.
New technology on the market supports progress in both risk adjustment optimization scope and capability, but complete solutions have not yet been widely adopted by payers. Furthermore, Gartner expects the need for risk adjustment optimization systems to increase over the next five years due to the growing prevalence of payer value-based provider reimbursement methodologies and purchaser needs to save money by fine-tuning payer premium payments.
User Advice: The risk adjustment optimization vendor space is highly fragmented, making selection more complex for payer CIOs. A large number of firms, ranging from small startups to major names, offer both point and complete end-to-end solutions. Vendors sell applications, as well as offering outsourced service models with a range of payment models. In addition, payers have few ways to validate vendor claims of incremental risk score improvements over an incumbent vendor or approach.
Payers must concentrate efforts in two areas in which vendor differentiations exist and offer meaningful risk score improvement:
- Analytics — Combining natural-language processing of unstructured text and clinician notes in medical records with learning algorithms to find more potential cases with coding gaps and increase success rate with each.
- Clinical data transfer — Obtaining medical records in a faster and more efficient manner to lower overall campaign cost and make follow-up on cases with smaller coding gaps more cost-effective through outright integration with provider electronic health record systems or tools to obtain clinical information digitally.
Finally, payers should seek vendors that distinguish themselves through:
- Development — Building a platform for future innovation and expansion, with a clear capability development roadmap in place for upcoming product enhancements.
- Integration — Linking data and workflows with risk assessment tools, population health, care management and quality applications to improve member medical management outcomes and organizationwide quality improvement goals.
Business Impact: Revenue enhancement opportunities from risk score optimization are substantial in Medicare Advantage and ACA commercial lines, and growing in managed Medicaid. Payers investing in improved risk adjustment management systems will see enhanced competitiveness and financial returns due to one or more of the following strategies:
- Identifying more cases with potential coding gaps, especially gaps that are less obvious and can only be found through a vendor's analysis of massive claim datasets across multiple payers to determine industrywide trends
- Better prioritizing cases for additional intervention, such as provider home visits
- Improving the throughput and efficiency of the overall risk adjustment campaign
- Lowering transaction costs for chart acquisition and clinical coding review
- Leveraging risk adjustment processes to complement quality improvement, large group underwriting and value-based provider contracting
Benefit Rating: Moderate
Market Penetration: 20% to 50% of target audience
Maturity: Early mainstream
Sample Vendors: Blue Health Intelligence; Health Fidelity; Indegene; Inovalon; Optum; Pulse8; Tessellate; Verscend
Appendixes
Figure 3. Hype Cycle for U.S. Healthcare Payers, 2016
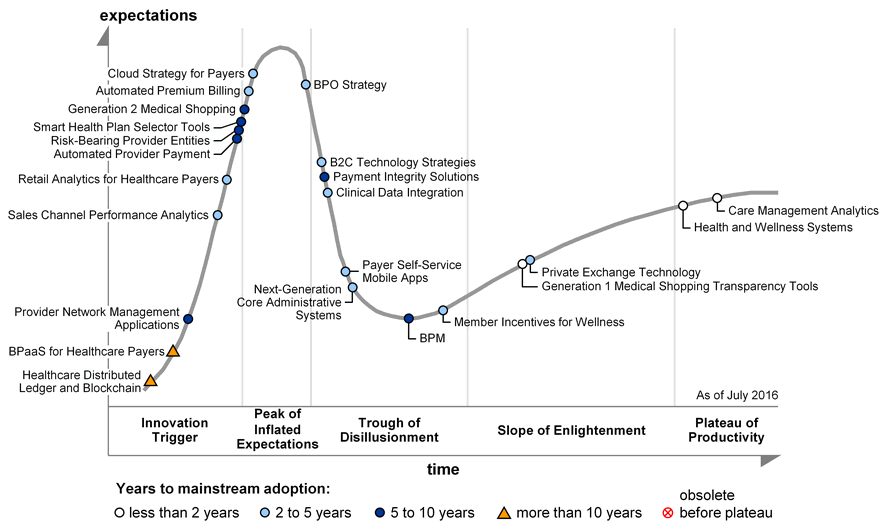
Source: Gartner (July 2016)
Hype Cycle Phases, Benefit Ratings and Maturity Levels
Table 1. Hype Cycle Phases
| Phase | Definition |
|---|---|
| Innovation Trigger | A breakthrough, public demonstration, product launch or other event generates significant press and industry interest. |
| Peak of Inflated Expectations | During this phase of overenthusiasm and unrealistic projections, a flurry of well-publicized activity by technology leaders results in some successes, but more failures, as the technology is pushed to its limits. The only enterprises making money are conference organizers and magazine publishers. |
| Trough of Disillusionment | Because the technology does not live up to its overinflated expectations, it rapidly becomes unfashionable. Media interest wanes, except for a few cautionary tales. |
| Slope of Enlightenment | Focused experimentation and solid hard work by an increasingly diverse range of organizations lead to a true understanding of the technology's applicability, risks and benefits. Commercial off-the-shelf methodologies and tools ease the development process. |
| Plateau of Productivity | The real-world benefits of the technology are demonstrated and accepted. Tools and methodologies are increasingly stable as they enter their second and third generations. Growing numbers of organizations feel comfortable with the reduced level of risk; the rapid growth phase of adoption begins. Approximately 20% of the technology's target audience has adopted or is adopting the technology as it enters this phase. |
| Years to Mainstream Adoption | The time required for the technology to reach the Plateau of Productivity. |
Source: Gartner (July 2017)
Table 2. Benefit Ratings
| Benefit Rating | Definition |
|---|---|
| Transformational | Enables new ways of doing business across industries that will result in major shifts in industry dynamics |
| High | Enables new ways of performing horizontal or vertical processes that will result in significantly increased revenue or cost savings for an enterprise |
| Moderate | Provides incremental improvements to established processes that will result in increased revenue or cost savings for an enterprise |
| Low | Slightly improves processes (for example, improved user experience) that will be difficult to translate into increased revenue or cost savings |
Source: Gartner (July 2017)
Table 3. Maturity Levels
| Maturity Level | Status | Products/Vendors |
|---|---|---|
| Embryonic |
|
|
| Emerging |
|
|
| Adolescent |
|
|
| Early mainstream |
|
|
| Mature mainstream |
|
|
| Legacy |
|
|
| Obsolete |
|
|
Source: Gartner (July 2017)